Nuclear Medicine
Marques Bradshaw
Blaine Mischen
The authors and editors acknowledge the contribution of the Chapter 5 authors from the second edition: Mark A. Auler, MD, and Kenneth Spicer, MD, and the Chapter 5 authors from the third edition: Beata Panzegrau, Phillip S. Davis, Leonie Gordon.
Case 5.1
HISTORY: A 68-year-old man with dementia, ataxia, and incontinence
 FIGURE 5.1.1 |
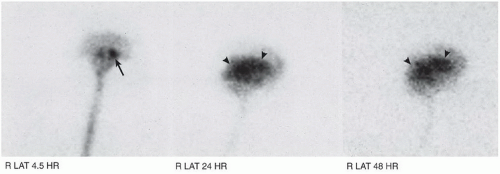 FIGURE 5.1.2 |
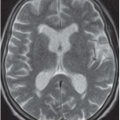
FINDINGS: Multiple frontal (Fig. 5.1.1) and lateral (Fig. 5.1.2) images from an indium-111 (111In) diethylenetriamine-penta-acetic acid (DTPA) cisternography study are presented. Activity is present in the basal cisterns at 4.5 hours (arrows). Mild lateral ventricular activity is also seen at this time and is more prominent at 24 and 48 hours (arrowheads). Flow over the convexities is delayed.
DIAGNOSIS: Normal-pressure hydrocephalus
DISCUSSION: Clinically, normal-pressure hydrocephalus is characterized by the triad of ataxia, dementia, and incontinence. Cerebrospinal fluid flow reversal is useful in distinguishing this entity from other causes of dementia associated with ventriculomegaly (i.e., hydrocephalus ex vacuo). Surgical shunting can alleviate a patient’s symptoms; however, not all patients respond to this treatment (1). The amount of response depends on the amount of activity in the ventricles compared with that over the convexities and on the duration of neurologic symptoms and signs (2).
Normally, the radiotracer reaches the basal cisterns within 1 hour after administration through lumbar puncture. Between 2 and 6 hours, the activity ascends into the interhemispheric and sylvian fissures. Radiotracer flows over the cerebral convexities by 24 hours. No lateral ventricular activity is seen under normal conditions. In classic normal-pressure hydrocephalus, radiotracer reflux into the lateral ventricles occurs and persists for 24, 48, or even 72 hours after injection.
Aunt Minnie’s Pearls
In normal-pressure hydrocephalus, radiotracer refluxes into the lateral ventricles and persists for 24, 48, or even 72 hours.
The clinical triad of dementia, ataxia, and incontinence is seen in normal-pressure hydrocephalus.
Case 5.2
HISTORY: A 62-year-old man who suffered a major cerebrovascular accident
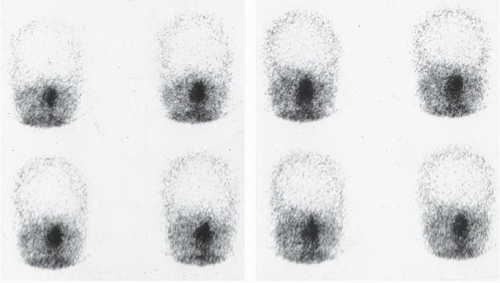 FIGURE 5.2.1 |
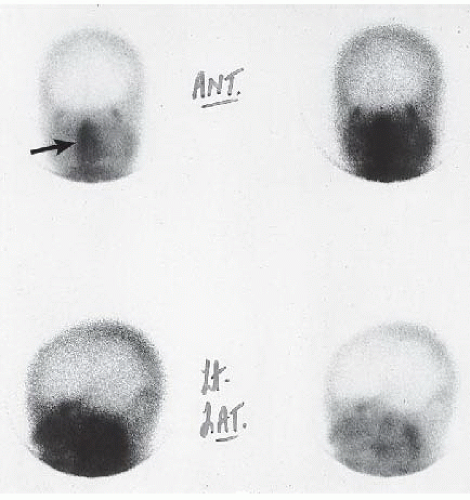 FIGURE 5.2.2 |
FINDINGS: The initial flow images from this technetium-99m (99mTc)-hexamethylpropylene amine oxime (HMPAO) cerebral perfusion study (Fig. 5.2.1) show that no arterial flow is present in either cerebral hemisphere. The delayed static images (Fig. 5.2.2) confirm that no cerebral activity is seen. Prominent activity is identified in the patient’s face and scalp (arrow).
DIAGNOSIS: Absent cerebral perfusion
DISCUSSION: Although the diagnosis of brain death is made on clinical criteria, the radionuclide cerebral perfusion study is often used for confirmation. Unlike electroencephalography, radionuclide evaluation does not produce false-positive studies in patients with hypothermia or a metabolic disturbance
(i.e., anoxia, uremia, hepatic encephalopathy, severe sepsis, or high doses of fentanyl, diazepam, or barbiturates) (3). The scintigraphic appearance of brain death involves absence of both intracranial arterial and major dural sinus flow. Controversy exists regarding whether faint visualization of the sagittal or transverse sinuses precludes this diagnosis (3). The hot-nose sign described with absent cerebral perfusion represents the shunting of blood from the internal to the external carotid arteries.
(i.e., anoxia, uremia, hepatic encephalopathy, severe sepsis, or high doses of fentanyl, diazepam, or barbiturates) (3). The scintigraphic appearance of brain death involves absence of both intracranial arterial and major dural sinus flow. Controversy exists regarding whether faint visualization of the sagittal or transverse sinuses precludes this diagnosis (3). The hot-nose sign described with absent cerebral perfusion represents the shunting of blood from the internal to the external carotid arteries.
Unlike DTPA, pertechnetate, and glucoheptonate, HMPAO is less dependent on bolus injection (3,4). Cerebral perfusion can be evaluated on static and on flow images because HMPAO normally crosses the blood-brain barrier.
Aunt Minnie’s Pearls
Absent cerebral perfusion can be accompanied by the hot-nose sign.
Nuclear studies are not limited by hypothermia or metabolic disturbance.
Case 5.3
HISTORY: A 69-year-old woman with a history of lung cancer and increased alkaline phosphatase
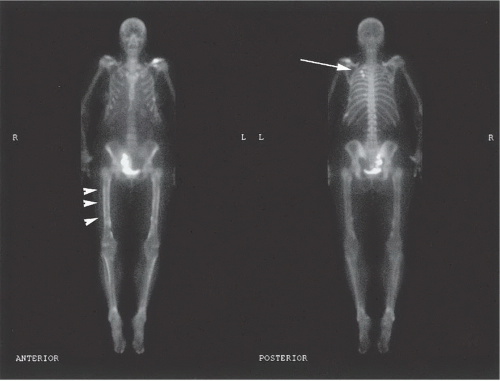 FIGURE 5.3.1 |
FINDINGS: Anterior and posterior whole-body images were obtained 3 hours after the administration of 25 mCi of 99mTc methylene diphosphonate (MDP; Fig. 5.3.1). The bone scan demonstrates multiple rib lesions consistent with a history of previous rib fractures; the string-of-pearls sign suggests traumatic injury to the ribs (arrow). Increased radiotracer uptake is identified along the cortices of both femurs and tibias bilaterally (arrowheads). Notice the uptake within the pelvis by a renal transplant.
DIAGNOSIS: Hypertrophic osteoarthropathy (HOA)
DISCUSSION: HOA is a syndrome characterized by scintigraphic and radiographic evidence of periosteal new bone formation. Clinically, the patient presents with digital clubbing, long-bone tenderness and pain, increased soft-tissue thickness, or asymmetric, arthritis-like changes within the limb joints (5). Secondary HOA is most commonly associated with an intrathoracic neoplasm (usually a bronchogenic carcinoma) or its metastases (6). The diaphyseal and metaphyseal regions of long bones are normally involved. Characteristically, a periosteal reaction (i.e., periostosis) occurs along the shafts of the femurs, tibias, ulnas, or radii. Skeletal scintigraphy demonstrates a characteristic pattern of uptake referred to as the double-stripe or parallel-track sign (7). This refers to the symmetric, diffuse uptake of radiotracer along the medial and lateral cortices of the long bones. Less commonly involved bones are the patella, scapula, clavicle, and skull.
Aunt Minnie’s Pearls
The double-stripe or parallel-track sign is characteristic of HOA.
HOA is typically seen in lung cancer.
Case 5.4
HISTORY: A 27-year-old woman with pain in the right hand who recently underwent open reduction and internal fixation of a distal right radial fracture
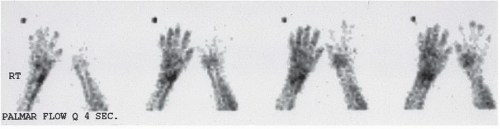 FIGURE 5.4.1 |
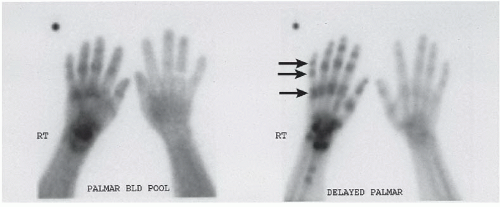 FIGURE 5.4.2 |
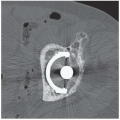
FINDINGS: Images from a three-phase bone scan demonstrate increased blood flow (Fig. 5.4.1) to the right wrist and hand. Immediate and delayed static images (Fig. 5.4.2) show diffuse increased bony uptake in a periarticular distribution (arrows). The two focal areas of abnormal increased activity in the distal right radius represent the region of fracture and operative fixation.
DIAGNOSIS: Reflex sympathetic dystrophy (RSD)
DISCUSSION: Patients with RSD (also called complex regional pain syndrome or Sudeck’s atrophy) present clinically with local pain, soft-tissue swelling, and vasomotor instability of the involved extremity. The most common causes of RSD include trauma (often minor), immobilization, infection, myocardial infarction, and neurologic disease (8). Symptoms are thought to occur because of an abnormal sympathetic nervous system response to the traumatic insult (9). The disorder is less common in children than in adults (10).
Radiographically, there is periarticular soft-tissue swelling and regional osteoporosis. Classically, bone scintigraphy demonstrates increased flow and periarticular uptake in the involved extremity, with delayed images being the most sensitive for the diagnosis of reflex sympathetic dystrophy. Radionuclide imaging is not as sensitive in diagnosing this entity if symptoms have been present for >1 year because delayed images may have normal or reduced activity (11).
Aunt Minnie’s Pearl
Increased flow + periarticular uptake + patient with history of trauma and vasomotor instability = RSD.
Case 5.5
HISTORY: A 69-year-old woman with an increased alkaline phosphatase level
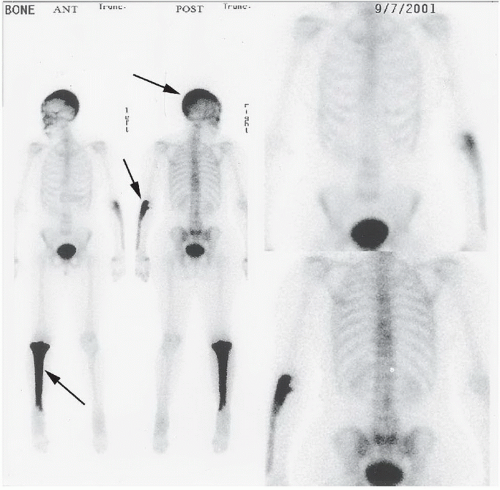 FIGURE 5.5.1 |
FINDINGS: Anterior and posterior whole-body images were obtained 3 hours after the administration of 25 mCi of 99mTc-MDP (Fig. 5.5.1). The bone scan demonstrates intensely increased radiotracer uptake within the right tibia, left ulna, and calvarium (arrows).
DIAGNOSIS: Paget’s disease
DISCUSSION: Paget’s disease is a metabolic disorder of bone that is caused initially by excessive resorption of bone followed by irregular deposition of “new” bone. Its incidence increases with age, and 3% of individuals older than 40 years of age are believed to have the disease (12). It is twice as common in the male population, and many patients are evaluated after an increase in serum alkaline phosphatase is incidentally discovered (13).
Paget’s disease can be monostotic or polyostotic and demonstrates intense radiotracer uptake within the bones involved. The characteristic uptake conforms to the shape of the bone that usually appears distorted or enlarged. The intense activity creates the appearance of an expanded cortex. Few other pathologic processes can create as intense a radiotracer uptake as Paget’s disease. The pelvis (hemipelvis) is the most commonly involved bone, followed by the spine, femur, skull, tibia, clavicle, and humerus (13).
Aunt Minnie’s Pearls
Extremely intense radiotracer activity that conforms to a distorted bone in a patient that is asymptomatic with increased alkaline phosphatase = Paget’s disease.
The most commonly involved bones are the pelvis, spine, skull, femur, scapula, tibia, and humerus.
Case 5.6
HISTORY: An 8-year-old girl with increased serum calcium and normal parathormone level
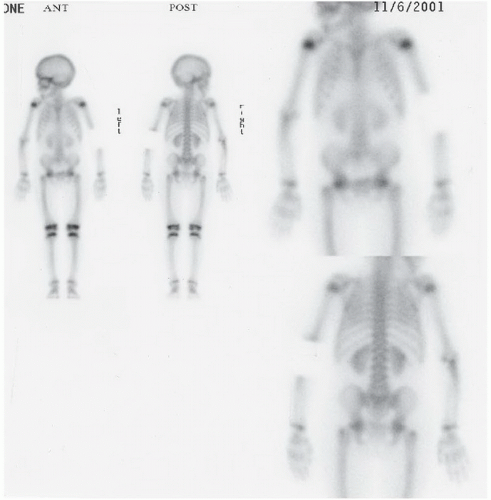 FIGURE 5.6.1 |
FINDINGS: Anterior and posterior whole-body images were obtained 3 hours after the administration of 12.5 mCi of 99mTc-MDP (Fig. 5.6.1). The bone scan demonstrates diffuse activity identified within both lungs.
DIAGNOSIS: Hypercalcemia
DISCUSSION: Diphosphonates are the primary ligands in skeletal scintigraphy. Extraosseous uptake of the bone-scanning agent is not unusual. The literature reports more than 20 causes of extraskeletal uptake (e.g., synovitis, bursitis, hematoma, fat necrosis, myositis ossificans, myocardial infarction, cerebral infarction, splenic infarction, effusion, ascites, edema) (14). When determining the significance of extraosseous uptake, it is important to identify the pattern of the uptake (i.e., focal or diffuse) and the structures involved.
Hypercalcemia causes a characteristic pattern of uptake within the soft tissues. Ordinarily, hypercalcemia produces diffusely increased radiotracer uptake within the lungs or stomach. Although this pattern is typical for hypercalcemia, the underlying cause can sometimes be elusive. Hypercalcemia is most commonly seen in hyperparathyroidism and neoplasms. Two other findings associated with hypercalcemia can be bilateral patellar uptake or diffuse calvarial and spinal uptake, sometimes referred to as the lollypop sign.
Aunt Minnie’s Pearls
Diffuse uptake in the lungs or stomach is typical of hypercalcemia.
Hypercalcemia is most commonly seen in hyperparathyroidism and neoplasms.
Case 5.7
HISTORY: A 10-week-old infant with cholestatic jaundice
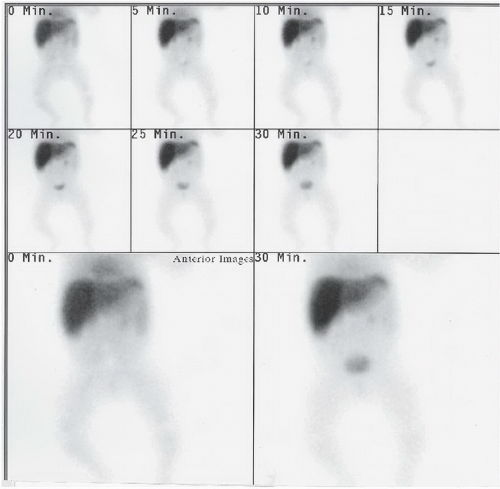 FIGURE 5.7.1 |
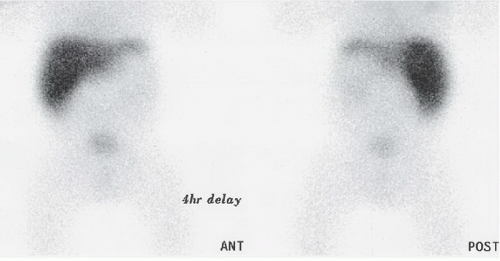 FIGURE 5.7.2 |
FINDINGS: Dynamic images of the upper abdomen were obtained at 5-minute intervals after the administration of 1.2 mCi of mebrofenin (Fig. 5.7.1). Delayed static images were performed at 2, 4, and 24 hours (Fig. 5.7.2). These images demonstrate activity within the liver and some activity within the kidney and bladder. No gallbladder or small-bowel activity is visualized.
DIAGNOSIS: Extrahepatic biliary atresia (EHBA)
DISCUSSION: EHBA is a congenital anomaly that leads to severe obstructive jaundice within the first 2 months of life. If untreated, it is universally fatal within 2 years (15). To avoid any irreversible damage, surgery is usually required within the first 60 days of life.
Biliary scans are an important diagnostic tool in excluding biliary atresia when it is suspected. Patient preparation is important and involves the administration of phenobarbital (2.5 mg/kg) for 5 days before the scan.
The demonstration of bowel activity by 24 hours effectively excludes biliary atresia from the differential diagnosis. Biliary scintigraphy is reported to have a sensitivity and specificity for EHBA of 88.2% and 88.9%, respectively (16). The absence of bowel activity by 24 hours does not always imply EHBA. Neonatal hepatitis (NH) can rarely demonstrate absent bowel activity by 24 hours. The degree of hepatocellular clearance as well as the hepatobiliary transit time of the agent can help in differentiating between EHBA and NH (16). However, further evaluation with ultrasound or biopsy is sometimes necessary to distinguish between NH and EHBA in equivocal cases.
Aunt Minnie’s Pearls
Bowel activity by 24 hours excludes biliary atresia.
If no bowel activity is demonstrated by 24 hours, consider ultrasound or biopsy to differentiate between EHBA and NH.
Case 5.8
HISTORY: A 30-year-old black man with cough and hilar adenopathy
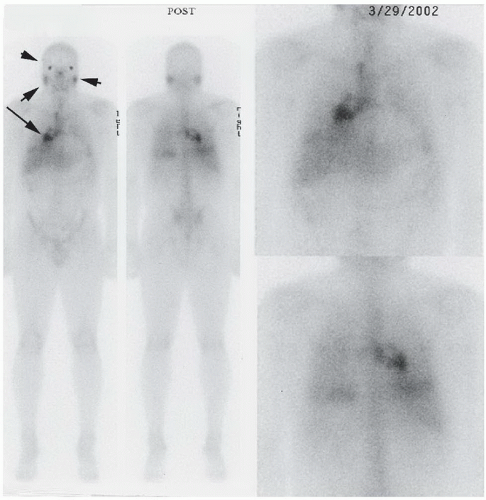 FIGURE 5.8.1 |
FINDINGS: Anterior and posterior whole-body images were obtained 48 hours after the administration of 8 mCi of gallium citrate (Fig. 5.8.1). These images demonstrate abnormal accumulation of radiotracer within the right paratracheal region and right hilum (arrow). Increased activity is visualized within the nasopharyngeal region and in the lacrimal and parotid glands (arrowheads). Some mild activity is visualized within the submandibular glands.
DIAGNOSIS: Sarcoidosis
DISCUSSION: Sarcoidosis is a chronic inflammatory disease that can involve any organ of the body. Gallium-67 has found favor in the imaging of sarcoidosis because of its avid accumulation at the sites of active disease. To diagnose sarcoidosis, one must combine radiographic and histologic information with the clinical findings. Although a diagnosis of sarcoidosis cannot be made by gallium scan alone, it provides important information to the clinician. It can serve as a guide to appropriate biopsies in patients clinically suspected of having active disease. Gallium scintigraphy is also helpful in distinguishing between active and inactive disease based on the degree of gallium-67 uptake. Gallium-67 is taken up only by active disease and not by fibrosis. It has proved beneficial in following
the progression of the disease and assessing its response to therapy.
the progression of the disease and assessing its response to therapy.
Findings on gallium-67 scintigraphy that are characteristic for active sarcoidosis are paratracheal uptake with bilateral hilar uptake that is in the shape of the Greek letter lambda. This is known as the “lambda” sign. Prominent gallium-67 uptake in the parotid, lacrimal, and salivary glands bilaterally is referred to as the “panda” sign. This is also commonly seen in patients with active disease. These two findings, when seen together, are highly specific for sarcoidosis (17).
Aunt Minnie’s Pearls
The lambda sign and panda sign = sarcoidosis.
Gallium-67 is the agent of choice for imaging sarcoidosis.
Case 5.9
HISTORY: A 41-year-old woman with hypercalcemia and increased parathormone
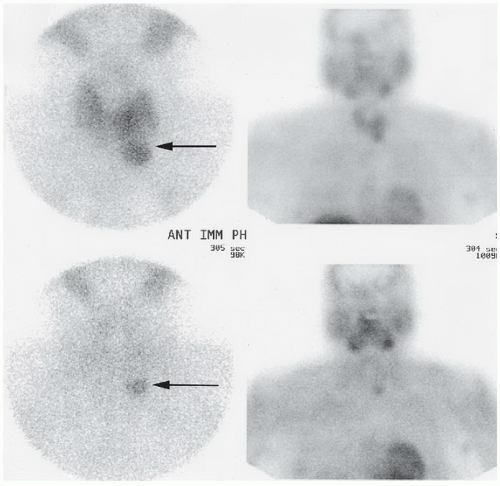 FIGURE 5.9.1 |
FINDINGS: Anterior and anterior oblique images of the thyroid were obtained at 20 minutes after the administration of 20 mCi of 99mTc-sestamibi (Fig. 5.9.1, upper images). These images demonstrate a focal area of increased radiotracer accumulation in the region of the left inferior pole of the thyroid gland (arrow). Anterior and anterior oblique images of the neck were obtained 2 hours after injection (Fig. 5.9.1, lower images) and demonstrate persistence of activity at the inferior pole of the left lobe of the thyroid while the remainder of the gland washes out (arrow).
DIAGNOSIS: Left inferior pole parathyroid adenoma
DISCUSSION: Parathyroid adenomas are responsible for primary hyperparathyroidism approximately 85% of the time (18). As many as 10% of these adenomas are ectopic (18). Surgery is the optimal treatment, for which accurate localization is essential. 99mTc-sestamibi is commonly used in the evaluation of parathyroid adenomas. Sestamibi localizes to mitochondria, which is found in greater concentrations in overactive parathyroid tissue than in the normal thyroid. There is consequently
slower washout of sestamibi from adenomas and hyperplastic parathyroid glands as compared with the surrounding thyroid tissue (19). Imaging at 20 minutes and then at 2 hours helps differentiate between the glandular tissues based on how quickly the radiotracer clears over time.
slower washout of sestamibi from adenomas and hyperplastic parathyroid glands as compared with the surrounding thyroid tissue (19). Imaging at 20 minutes and then at 2 hours helps differentiate between the glandular tissues based on how quickly the radiotracer clears over time.
A parathyroid adenoma typically demonstrates a focus of increased activity that persists even at 2 hours after injection. The remainder of the thyroid and parathyroid should wash out. A subtraction method is also commonly employed in parathyroid imaging. With this method, a thyroid agent (e.g., pertechnetate) is subtracted from a sestamibi or thallium scan. Persistent activity is likely the result of overactive parathyroid tissue. The latter method is slightly more sensitive than the differential washout method, with a reported sensitivity of 90% (20).
Aunt Minnie’s Pearl
A focal hot spot that persists with delayed washout of sestamibi is characteristic of a parathyroid adenoma.
Case 5.10
HISTORY: An infant with hypothyroidism
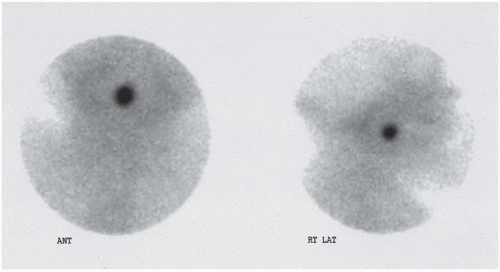 FIGURE 5.10.1 |
FINDINGS: A focal area of increased activity is present in the midline in the region of the tongue base on anteroposterior (ANT) and right lateral (RT LAT) views from a 99mTc-pertechnetate thyroid scan (Fig. 5.10.1). No activity is seen in the thyroid bed.
DIAGNOSIS: Lingual thyroid
DISCUSSION: Lingual thyroid results from failure of the thyroid gland to descend during embryogenesis. The ectopic gland is typically hypofunctional. Hypothyroidism associated with ectopic thyroid tissue occurs sporadically, whereas hypothyroidism from biosynthetic defects is inherited (21). In addition to hypothyroidism, the lingual thyroid may present as a mass in the tongue or upper neck. This abnormality must be diagnosed shortly after birth because failure to promptly begin replacement therapy adversely affects intellectual development.
Aunt Minnie’s Pearls
An ectopic or lingual thyroid is typically hypofunctional.
Screening for hypothyroidism is routine in newborns because failure to diagnose hypothyroidism may result in severe intellectual impairment.
Case 5.11
HISTORY: A 40-year-old woman with hypertension refractory to medical therapy
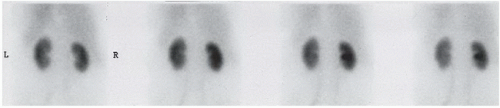 FIGURE 5.11.1 |
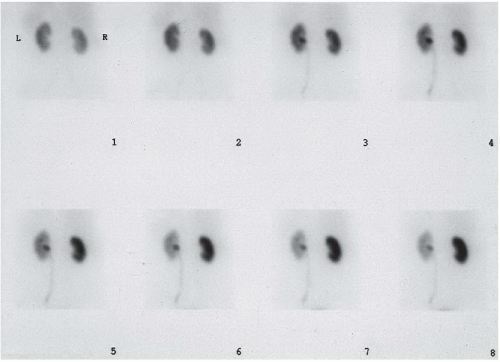 FIGURE 5.11.2 |
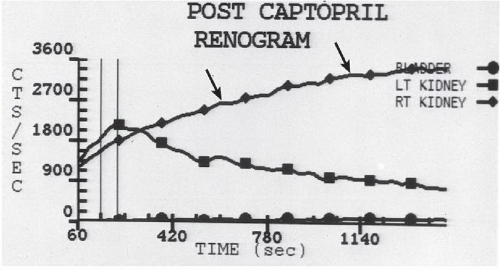 FIGURE 5.11.3 |
FINDINGS: Images acquired during a precaptopril 99mTc-MAG3 renogram (Fig. 5.11.1) demonstrate slightly increased cortical activity retention in the right kidney. After captopril administration (Fig. 5.11.2), this asymmetry becomes pronounced. Right renal cortical activity retention is significant, and excretion of radiopharmaceutical into the collecting system is minimal. The abnormal response of the right kidney to captopril administration is also demonstrated on a time-activity curve of the renogram (Fig. 5.11.3, arrows).
DIAGNOSIS: Right renovascular hypertension
DISCUSSION: Renovascular hypertension is caused by hypoperfusion-induced stimulation of the renin-angiotensin system. It accounts for approximately 1% to 2% of all hypertensive patients (22). The most common causes of renal hypoperfusion are atherosclerosis and fibromuscular dysplasia. The involved kidney maintains glomerular filtration rate by compensatory vasoconstriction of the efferent arteriole by angiotensin II, the end product of the renin-angiotensin system. Captopril, an inhibitor of angiotensin-converting enzyme, prevents efferent arteriole constriction. If a hemodynamically significant lesion of the renal artery is present, the glomerular filtration rate will drop on administration of captopril compared with the precaptopril examination. Scintigraphically, this difference is seen as delayed radiotracer uptake and cortical retention (23).
Aunt Minnie’s Pearls
Renovascular hypertension is mediated by the renin-angiotensin system.
After captopril administration, delayed radiotracer uptake and cortical retention are seen in the affected kidney.
Case 5.12
HISTORY: A decreased urine output after renal transplantation
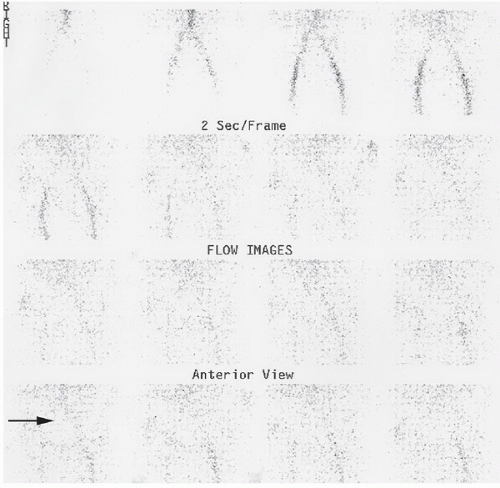 FIGURE 5.12.1 |
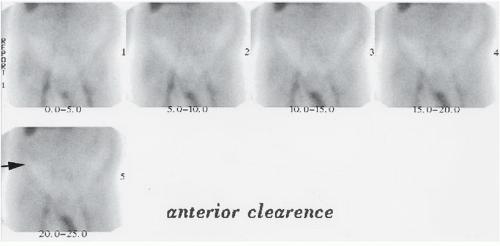 FIGURE 5.12.2 |
FINDINGS: Dynamic flow images of the lower abdomen and pelvis were obtained at 2-second-per-frame intervals after the intravenous administration of 8 mCi of 99mTc-mertiatide (Fig. 5.12.1). These images demonstrate no flow of radiotracer to the renal transplant (arrow).
Dynamic clearance images reveal no uptake or excretion of the radiotracer (Fig. 5.12.2). Rather, a photopenic region (arrow) is visualized within the right anterior iliac fossa where the renal transplant is presumably located.
DIAGNOSIS: Vascular obstruction (i.e., renal artery obstruction)
DISCUSSION: Renal scintigraphy is valuable in the evaluation of complications associated with renal transplantation. In the immediate postoperative period (<1 week), a number of problems can occur, including hyperacute rejection, accelerated rejection, renal vein thrombosis (RVT), renal artery thrombosis (RAT), urinary leak, edema, and a hematoma. RAT and RVT are likely the result of surgical complications. The renal allograft contains no venous collaterals. A thrombus in the renal vein can result in an outflow obstruction that leads to increased impedance and ultimately to arterial compromise. RVT and RAT have the same clinical significance and can appear similar with scintigraphic examination (24).
In vascular obstruction, there is no flow, uptake, or excretion of the radiotracer, causing a photopenic defect within the expected location of the renal transplant. The defect is enhanced by normal background activity.
Hyperacute rejection would look similar, although this diagnosis is usually made in the operating room. In hyperacute rejection, preformed antibodies attack the transplanted kidney, causing vascular compromise and inhibiting flow to the kidney. The kidney turns blue immediately in the operating room.
Aunt Minnie’s Pearls
No flow, no uptake, and no excretion in the immediate postoperative period = vascular occlusion.
RAT and RVT look similar scintigraphically.
Case 5.13
HISTORY: A 39-year-old man with an acute onset of chest pain and dyspnea
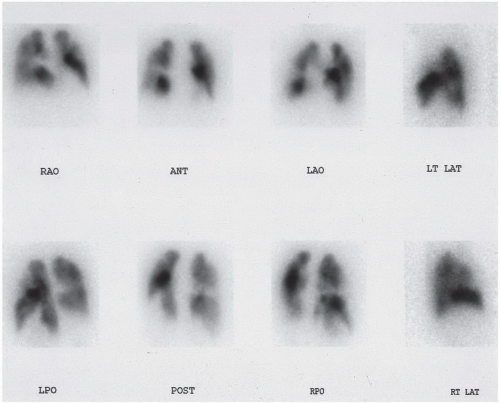 FIGURE 5.13.1 |
FINDINGS: Pulmonary perfusion images obtained after injection of 99mTc-MAA (Fig. 5.13.1) reveal multiple, segmental perfusion defects. Posterior ventilation images using xenon-133 (133Xe; Fig. 5.13.2) demonstrate normal ventilation during first breath, equilibrium, and washout images.
DIAGNOSIS: Multiple pulmonary emboli
DISCUSSION: Pulmonary embolic disease is typically a sequela of deep venous thrombosis. Patients can present with a multitude of nonspecific findings, including pleuritic chest pain, hemoptysis, dyspnea, hypoxia, and tachypnea. Radiographic analysis is often nonspecific, with findings including a normal chest, atelectasis, and small pleural effusion. Less commonly, focal oligemia (i.e., Westermark sign), pulmonary artery enlargement, or a pleural-based, wedge-shaped density indicative of pulmonary infarction (i.e., Hampton’s hump) can be seen.
If multiple (2) segmental ventilation-perfusion mismatches are identified in areas where there is no corresponding chest radiographic abnormality, pulmonary embolism is diagnosed with high probability
in all classification schemes. In rare cases, vasculitides can produce a similar pattern with segmental mismatches in several lobes of the lung, but the patient’s clinical presentation and medical history should allow accurate diagnosis of these patients. Prospective investigation of pulmonary embolism diagnosis (PIOPED) investigators have updated diagnostic criteria for probability of pulmonary embolus (25), and this source offers further discussion.
in all classification schemes. In rare cases, vasculitides can produce a similar pattern with segmental mismatches in several lobes of the lung, but the patient’s clinical presentation and medical history should allow accurate diagnosis of these patients. Prospective investigation of pulmonary embolism diagnosis (PIOPED) investigators have updated diagnostic criteria for probability of pulmonary embolus (25), and this source offers further discussion.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


