Other Oncology
QUESTIONS
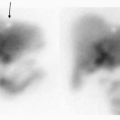
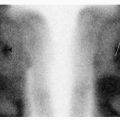
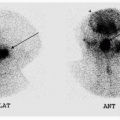
1 Which of the following interventions would LEAST likely help in reducing the abnormal F-18 FDG uptake seen in the following patient?
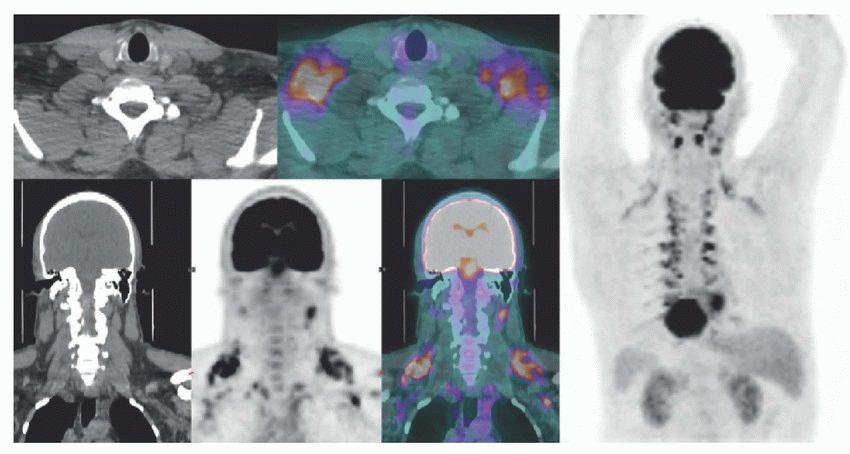 |
A. Beta-blockers such as propranolol
B. Raising the ambient temperature
C. Phenylephrine
D. Diazepam
View Answer
1 Answer C. The supplied images demonstrate intense FDG uptake in bilateral cervical, supraclavicular, subpectoral, and paravertebral regions corresponding to fat attenuation on CT scan. Findings are consistent with physiologic brown adipose tissue (BAT) uptake. BAT is a sympathetically innervated tissue that plays an important role in cold-induced and diet-induced thermogenesis. Physiologic BAT uptake is typically identified in bilateral cervical, supraclavicular, axillary, subpectoral, costovertebral, and retroperitoneal/retrocrural regions. It occurs more commonly in cold weather, young females, and children. Successful strategies to reduce brown fat uptake include preventing exposure to cold temperature, controlling environment temperature prior to and after FDG injection (warm clothing, warm blankets, temperature-controlled rooms at 75°F, etc.), avoiding sympathetic stimulants (nicotine, phenylephrine, ephedrine, etc.), pharmacologically by reducing synthetic activity (beta-blockers such as propranolol), or pharmacologically by using sedatives such as oral or intravenous diazepam. In a study done by Agrawal et al., 40 mg propranolol PO administered 60 minutes prior to F-18 FDG injection resulted in complete resolution of brown fat uptake in 90% of patients. Although mixed results have been reported with the success of diazepam in reducing BAT uptake, Rajan et al. observed a significant reduction in brown fat activity following premedication with 5 mg of diazepam intravenously 10 minutes prior to F-18 FDG administration. Sympathetic stimulants such as phenylephrine are known to cause brown fat activation and increase its FDG uptake.
References: Agrawal A, Nair N, Baghel NS. A novel approach for reduction of brown fat uptake on FDG PET. Br J Radiol 2009;82(980):626-631.
Garcia C, Bandaru V, Van Nostrand D, et al. Effective reduction of brown fat FDG uptake by controlling environmental temperature prior to PET scan: an expanded case series. Mol Imaging Biol 2010;12(6):652-656.
Rakheja R, Ciarallo A, Alabed YZ, et al. Intravenous administration of diazepam significantly reduces brown fat activity on 18F-FDG PET/CT. Am J Nucl Med Mol Imaging 2011;1(1):29-35.
2 With regard to breast cancer, F-18 FDG is LEAST likely to be helpful in which of the following clinical scenarios?
A. Initial staging in patients with advanced breast cancer
B. Evaluation of lymph node status in a patient with newly diagnosed breast cancer
C. Evaluating the response to treatment in locally advanced and metastatic breast cancer
D. Staging recurrent or metastatic breast cancer
View Answer
2 Answer B. Sentinel node localization with Tc-99m sulfur colloid, with or without blue dye, is the preferred method for evaluating non-palpable lymph nodes in a patient with newly diagnosed breast cancer. Since a negative F-18 FDG-PET scan does not exclude the need for further workup, it has no role in this scenario. Mammography, MRI, and ultrasound are the primary modalities used in screening and diagnosing breast cancer. F-18 FDG-PET is most useful in the initial staging of patients with advanced breast cancer, in monitoring response to therapy, and in the evaluation of patients with suspected recurrence.
References: Rosen EL, Eubank WB, Mankoff DA. FDG PET, PET/CT, and breast cancer imaging. RadioGraphics 2007;27(suppl 1):S215-S229.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:254-256.
3 Which of the following statements is MOST correct regarding the preparation instructions for a patient undergoing F-18 FDG-PET/CT for tumor imaging?
A. The patient should fast for 12 to 24 hours prior to the examination.
B. Hydration with dextrose containing solutions does not need to be discontinued.
C. Diabetic medications should be discontinued for 12 hours prior to the examination.
D. Strenuous exercise should be avoided for 24 hours prior to the FDG-PET/CT examination.
E. The fasting blood glucose levels should be <250 mg/dL prior to the injection of FDG.
View Answer
3 Answer D. Patient preparation is critical for individuals undergoing evaluation of malignancy by FDG-PET/CT. The goal of patient preparation is to maximize the F-18 FDG uptake by tumor and minimize the normal physiologic uptake in other tissues. The patient should be instructed to fast and not consume beverages, except for water, for at least 4 to 6 hours before the administration of F-18 FDG to decrease physiologic glucose levels and to reduce serum insulin levels. Similarly, IV fluids containing dextrose or parenteral feedings should be withheld for 4 to 6 hours. Since tumor uptake of F-18 FDG is reduced in hyperglycemic states, most institutes reschedule patients if the blood glucose level is >200 mg/dL. Both NCI and ACR recommend avoiding strenuous activities such as jogging, cycling, weight lifting, strenuous housework, and sexual activity for a minimum of 24 hours in order to reduce physiologic muscular uptake. All oral medications, including those for diabetes, can be taken as prescribed. While there are no current guidelines, at our institution patients taking long-acting insulin at night before the study are instructed to take half the dose to avoid an episode of hypoglycemia from a full dose.
Reference: Surasi DS, Bhambhvani P, Baldwin JA, et al. (1)(8)F-FDG PET and PET/CT patient preparation: a review of the literature. J Nucl Med Technol 2014;42(1):5-13.
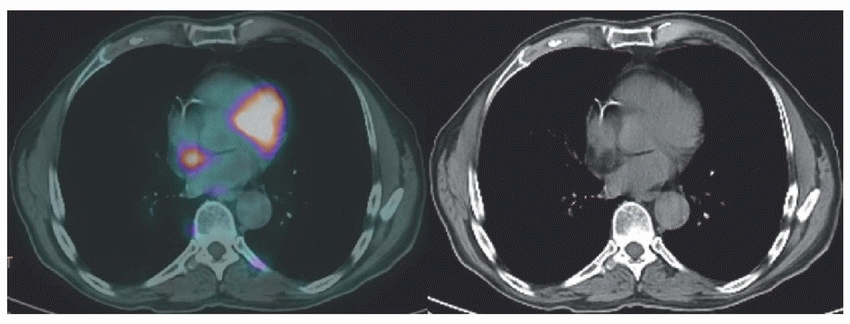
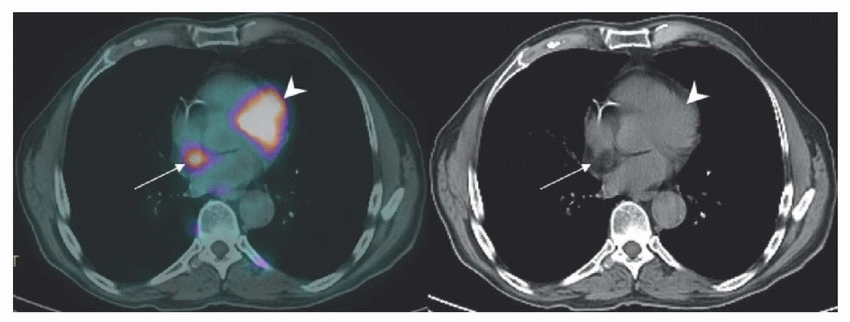
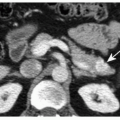
4 The following FDG-PET/CT images were acquired from a patient with a clinical history of head and neck squamous cell carcinoma. What is the most likely etiology of the abnormal intracardiac uptake?
 |
A. Atrial thrombus
B. Ventricular thrombus
C. Primary cardiac malignancy
D. Infectious endocarditis
E. Physiologic
F. Metastasis
G. Sarcoidosis
View Answer
4 Answer E. Axial fused F-18 FDG-PET/CT and CT images demonstrate a moderate-sized focus of intense FDG uptake corresponding to fat attenuation between left and right atrium (arrow). This is physiologic FDG uptake within lipomatous hypertrophy of the interatrial septum. Lipomatous hypertrophy of the intracranial septum may demonstrate variable degree of FDG uptake. This patient also had significant BAT uptake elsewhere in the body, and intense uptake within this lipomatous hypertrophy of interatrial septum is likely secondary to BAT within it. A large focus of intense activity in the location of the left ventricle (arrowhead) is physiologic glucose uptake in the anterior wall of the myocardium. Depending on the patient’s nutritional status, myocardium can utilize either fatty acids or glucose for metabolism and demonstrate a variable degree of F-18 FDG uptake.
 |
Reference: Rao PM, Woodard PK, Patterson GA, et al. Myocardial metastasis or benign brown fat? Circ Cardiovasc Imaging 2009;2(4):e25-e27.
5 F-18 FDG-PET can be false negative in the evaluation of which of the following malignancies?
A. Squamous cell carcinoma of the head and neck
B. Squamous cell carcinoma of the lung
C. Esophageal adenocarcinoma
D. Adenocarcinoma of the lung
E. Small cell lung carcinoma
F. Lung carcinoid
View Answer




5 Answer F. Tumors with low metabolic activity such as bronchioloalveolar carcinoma and carcinoid tumors can give rise to false-negative PET results. A well-differentiated lepidic predominant adenocarcinoma can also be falsely negative on FDG-PET. FDG-PET has been reported to have false-negative results with mucosa-associated lymphoid tissue (MALT), extranodal marginal zone lymphoma, and chronic lymphocytic leukemia (CLL). However, FDG-PET has been found to be useful in the detection of Richter’s transformation of CLL to large cell lymphoma with a high sensitivity and specificity and negative predictive value. Lesions <1 cm in diameter may be below PET resolution and can be falsely negative on FDG-PET.
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
