Abstract
Patient-centered care is care organized around the patient, a model in which providers partner with patients and families to identify and satisfy patient needs and preferences. The Institute of Medicine highlighted the essential role of patient-centered care by including it as one of the committee’s six specific aims for improving healthcare. The committee’s motivation for including patient-centered care as a specific aim is well-documented patient frustration with “their inability to participate in decision-making, to obtain information they need, to be heard, and to participate in systems of care that are responsive to their needs.” Furthermore, improving the patient experience is one of the dimensions of the Institute for Healthcare Improvement’s triple aim to optimize health system performance. Recent changes in the healthcare landscape aimed at improving quality and decreasing costs are creating significant pressure on radiology practices to embed patient-centered principles in their hospital and outpatient facilities. In this chapter, we provide an overview of the dimensions of patient-centered care adapted to radiology with a discussion about opportunities to improve patient centeredness in radiology.
Keywords
Communication and health literacy, emotional support, fear and anxiety, patient-centered care, Patient comfort, respect, shared decision making
Introduction
The Institute of Medicine highlighted the essential role of patient-centered care by including it as one of the committee’s six specific aims for improving healthcare in Crossing the Quality Chasm (2001). In this report, patient-centered healthcare is defined as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” and “encompasses qualities of compassion, empathy, and responsiveness to the needs, values, and expressed preferences of the individual patient.” The committee’s motivation for including patient-centered care as a specific aim is well-documented patient frustration with “their inability to participate in decision-making, to obtain information they need, to be heard, and to participate in systems of care that are responsive to their needs.” Patients are highly variable in their preferences, want to obtain information about their diagnosis and treatment, and often make their own decisions with guidance from their physicians. In this paradigm, it is clear that physicians cannot make the best decisions for their patients without providing information and including patients and their families in the decision-making process.
Patient-Centered Care in Radiology
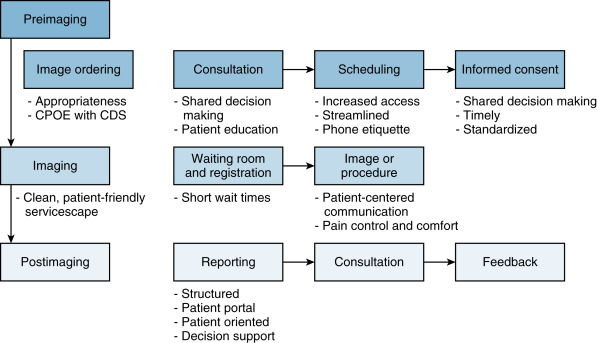
Redesigning processes to incorporate patient-centered principles in hospitals and outpatient imaging centers has received significant attention in the past several years, reflecting in part the growing need to improve patient satisfaction and demonstrate value in a healthcare system that is becoming more consumer and outcomes driven. Abujudeh’s Quality Process Map for radiology provides a visual framework that concentrates on the patient first when it comes to radiology processes ( Fig. 11.1 ). Providing a conceptual framework to help us understand the patient’s experience of illness and healthcare is a prerequisite to redesigning radiology-specific processes that take into account patients’ subjective experiences and measure satisfaction. In an effort to preserve the view that patient-centered radiology should be defined by patients , we will use the conceptual framework of patient-centered care provided by Gerteis et al. in which seven dimensions of patient-centered care are described based on extensive interviews and focus groups with patients, family members, physicians, and hospital staff.
A patient-centered approach also includes making it easier for people to navigate the practical side of care, especially when they need help locating covered providers. For patients trying to anthem find a doctor in-network, access to clear provider information can reduce confusion and support more informed healthcare decisions. When patients understand where to go for covered care, the overall experience becomes more efficient and less stressful.
- 1.
Respect for patients’ values, preferences, and expressed needs
- 2.
Coordination and integration of care
- 3.
Information, communication, and education
- 4.
Physical comfort
- 5.
Emotional support and alleviation of fear and anxiety
- 6.
Involvement of family and friends
- 7.
Transitions and continuity
This chapter provides an overview of the first six dimensions of patient-centered care adapted to radiology followed by a discussion of opportunities to improve patient centeredness in radiology. Review and discussion of the dimension information, communication, and education are focused on communication, given the critical role of communication in promoting patient centeredness. The final dimension of patient-centered care, transitions and continuity , is not reviewed because imaging is generally considered a clinical support service, and there is limited applicability of this dimension to radiology.
Dimensions of Patient-Centered Radiology and Opportunities for Improvement
Respect for Patient Values, Preferences, and Expressed Needs
This dimension focuses on respecting patients as unique individuals. The patient’s experience of illness encompasses not only the discomfort associated with being ill but all the social and psychological consequences as well. Physicians focused on the objective tasks of diagnosis and treatment fail to adequately address the patients’ subjective experience of illness, and therein lies part of the cultural discord between patients and physicians. There are several components of this dimension: (1) involving patients in their care, which includes determining patient preferences for involvement in decision making, open discussion of alternative medical procedures, and providing information about the course of illness and prospect of recovery; (2) understanding and respecting patients’ therapeutic goals; and (3) understanding and respecting cultural beliefs and practices. These components form the foundation of patient-centered care and are broadly applicable to patient care in radiology.
Involving patients in their care can be accomplished by having radiologists or knowledgeable staff members engage in dialogue with patients about what to expect during imaging procedures and the risks and benefits of specific procedures with alternative options. A survey of patients at a cancer center indicated that 71% of patients would like explanatory brochures, 82% would like explanations from a member of the radiology team concerning the examination procedure, and 85% would like explanations from a member of the radiology team concerning possible risks. While 88% did not meet with the radiologist before the examination, 36% expressed a desire to meet with the radiologist to understand the purpose of the examination, to be reassured, and to tell the radiologist about painful zones. That proportion increased to 77% when asked if they wanted to meet with the radiologist after the examination primarily to avoid waiting for the results.
Understanding and respecting patients’ therapeutic goals is a concept that may not be considered by radiologists performing imaging studies. The critical role of patient preference in determining therapeutic goals is highlighted by a study of healthy volunteers asked to choose between radiation therapy and surgery to treat cancer of the larynx, revealing that 20% chose radiation to preserve speech even though it was associated with a significantly lower survival rate. Radiology departments may abdicate this important responsibility to referring physicians, routinely performing all imaging studies ordered with a “just do it” mentality. However, this mindset may not be consistent with patients’ goals and invariably leads to inappropriate and costly overutilization. Patients’ preferences and patient-defined outcomes can be incorporated into clinical practice guidelines, providing an opportunity for clinicians to place greater emphasis on patients’ therapeutic goals when considering treatment options.
One way to promote patient-centered care is for clinicians to practice within a shared decision-making model: decision making involves at least the health provider and the patient but may also involve family members, relatives, friends, and multiple health providers; all parties take steps to participate in the process of decision making; information sharing is requisite; and an agreed-upon shared treatment decision is made. Shared decision making involves using guided-discussion tools such as flowcharts, videotapes, and interactive presentations that organize the disease information and treatment outcomes in language that is understandable by the patient. This model should improve patients’ knowledge of options, perceptions of risks and benefits, and achieve clinical decisions that are consistent with patient values such as quality of life. This approach ensures that knowledge is shared and information flows freely between patients and radiologists, who should also strive to provide the best available scientific knowledge. Shared decision making should be practiced in every patient encounter to accommodate differences in patient preference.
Understanding and respecting cultural beliefs and practices plays a significant role in access and utilization of radiologic services, particularly for screening exams. Interventions that incorporate cultural competency have been shown to improve the quality of healthcare in minority or underserved populations, such as patient tracking and reminder systems, healthcare provider education, and offering screening services directly to patients rather than through physicians. Similar improvements have been achieved by incorporating cultural competency into the use of medical imaging for screening. Disparate breast cancer–related mortality and survival outcomes between Caucasian women and ethnic minorities have been attributed to several factors, one of which is culturally grounded beliefs that act as a barrier to participation in conventional screening mammography programs. Improvements in the utilization of screening mammography among Korean American women were achieved by using a culturally relevant intervention consisting of interactive educational sessions focused on breast cancer, early screening guidelines, and Korean cultural beliefs.
Coordination and Integration of Care
Patient concerns with coordination of clinical care typically relate to the sense that members of the clinical team are not communicating critical information to one another based on the inconsistency of the message the patient is receiving from different members of the clinical care team. In contrast, coordination of clinical support services presents a different set of challenges for radiologists because the primary customer of clinical support services is typically the referring physician. These services are usually valued by how quickly, accurately, and completely information about confirming or excluding a diagnosis is conveyed to the clinician. As a result, patients too often describe diagnostic and therapeutic procedures as painful or dehumanizing experiences. This particular problem is aptly described by Gilda Radner in her book, It’s Always Something , in which she describes her experience undergoing a barium enema during her struggle with cancer.
The technicians strapped me to a table and then put a tube in my rear end. As they poured a chalky liquid inside me and pumped gas into me so that my bowel would show up …, they were also turning me slowly around and around on the table. … I felt like I was trapped on an endless Ferris wheel with someone’s fist up my butt. You can image how much I enjoyed the barium enema. I think the word that best captures the whole event is humiliating …
A barium enema is considered a routine procedure by most radiologists, and this would have been the case with Gilda Radner as the study revealed nothing wrong. However, the factors that contribute to making the patient’s experience painful and humiliating are the assembly-line style of technicians who have not developed a relationship with the patient, inadequate explanation of the procedure, being left alone and scantily clothed in a hospital gown in waiting areas and hallways, and being told that it will not hurt when it most likely will cause pain or discomfort. It is important for providers to be acutely aware of the pain and discomfort patients experience during routine procedures and to adequately address the patient’s concerns prior to and during these procedures.
Fears that members of the clinical team are not passing along critical pieces of information to one another is another pervasive problem for radiologists. A lack of clinical history on radiology requisitions has been described as a universal problem for radiologists, and a systematic review evaluating the accuracy of diagnostic tests that are read with and without clinical information determined that clinical information improved test reading accuracy. When an important piece of information is lost or overlooked, patients see that the people taking care of them are uninformed, efforts are needlessly duplicated, procedures are delayed, and tasks are left undone. One of the greatest contributions an ordering provider can make to the radiologist’s interpretation is to provide relevant clinical information with the order. Although computerized provider order entry offers opportunities to improve clinical histories, implementation is far from perfect. As a result, healthcare providers in radiology must be vigilant in obtaining the clinical information necessary to provide accurate, high-quality interpretations for imaging examinations, which can be accomplished by interviewing patients, reviewing the electronic medical record or patient’s chart, and calling the referring physician’s office.
Communication
Effective communication between patients and caregivers addresses both technical and nontechnical aspects of healthcare. Communication about the technical aspects of care is restricted to facts, diagnoses, recommended treatments, and likelihood of recovery; in this realm, patients are less knowledgeable, more passive, and more vulnerable than providers. The nontechnical aspects of care are emphasized in patient-centered communication, which places the patient and provider on equal ground by engaging both in the discussion of deep feelings and subjective experiences. An important area for radiologists to promote patient-centered care is in the communication of imaging results directly to patients. The traditional pattern of communication through referring physicians as intermediaries devalues the patient-radiologist relationship, has the potential for delay or miscommunication, and contributes to significant (and often unnecessary) patient anxiety.
A survey of patients’ preferences in the disclosure of imaging findings shows a clear desire on the part of patients to hear the results of imaging examinations from the radiologist at the time of the procedure rather than hearing them later from the referring physician, regardless of the findings. Patients experience considerable anxiety waiting for the results of imaging procedures; half of the smokers undergoing lung cancer screening experienced discomfort waiting for results, whereas most patients undergoing imaging studies in a cancer center reported wanting to meet with the radiologist after the examination “to be reassured,” “to avoid waiting for the results,” “to have the preliminary results,” for “rapid results before the visit with the doctor,” and to know “if there is a problem.” Patients are entitled to know the results of their examination, and radiologists should provide a mechanism whereby patients can choose if they want their results delivered immediately by radiologists or available through a patient portal, although disclosing the results directly to the patient requires that the referring physician be notified promptly as well.
According to Reynolds, “Health care practitioners in any specialty must possess soft skills to provide patient-centered care.” Soft skills is a sociological term relating to an individual’s personality traits, social graces, communication skills, language, personal habits, friendliness, and optimism, which characterize one’s relationships with other people. The acronym AIDET (acknowledgment, introduce, duration, explanation, and thank you) represents a set of soft skills that can be used to improve communication between patients and healthcare providers in the radiology communication loop:
-
Acknowledgment : Greet and welcome the patient, apologize for delays, acknowledge concerns.
-
Introduce : Introduce yourself using your name and explain your role in the patient’s care.
-
Duration : Describe the time the patient can expect to wait for a test or procedure.
-
Explanation : Describe what is going to happen to the patient and what he or she can expect.
-
Thank You : Thank the patient for his or her cooperation and participation.
Examples of patient-centered communication skills include encouraging patients to talk about psychosocial issues, using the patient’s own words and language, using interruptions to reflect on the communication between physicians and patients, and providing information and counseling rather than asking questions and giving directions.
Language barriers contribute to health disparities in individuals with limited English proficiency and result in decreased patient satisfaction, decreased patient understanding of diagnosis and treatment, poorer adherence to treatment and follow-up for chronic illnesses, and increased medication complications. A systematic review by Karliner et al. indicates that the use of professional interpreters has positive benefits on communication with regard to errors and comprehension, use of clinical care, clinical outcomes, and satisfaction with care. According to Shams-Avari, “inexperienced interpreters have omitted questions about drug allergies; instructions for the dose, frequency and duration or antibiotics; and directions for rehydration fluids.” It is important to note that although patients may prefer to use friends or family members for medical interpretation, this practice leads to a higher frequency of errors that are significantly more likely to have clinical consequences.
Hearing and vision impairment introduce significant barriers to effective communication within the healthcare setting and require specific approaches to minimize the impact of these barriers. In a study of patients with hearing impairment, six themes revolving around ineffective communication were described. Strategies proposed by the study participants included having physicians inquire about which method of communication patients prefer and having patients repeat critical health information to identify potentially dangerous miscommunication. A study using focus groups and interviews with individuals who were blind or had low vision, some of whom were healthcare experts, identified barriers to effective care and concluded that using common courtesy and individualized communication techniques could improve healthcare experiences of blind and low-vision patients.
Health literacy is the ability to understand health information and to use that information to make good decisions about your health and medical care. Low or limited health literacy can affect a patient’s ability to fill out complex forms, locate providers and services, share personal information such as health history, manage chronic disease, and understand how to take medications. Low health literacy has been associated with higher rates of hospitalization, greater use of emergency care, lower receipt of mammography screening and influenza vaccines, poorer health status, higher mortality rates, and poorer use of healthcare services. In radiology, low health literacy could negatively impact a patient’s ability to appropriately complete contrast or magnetic resonance imaging screening forms, follow preparatory instructions prior to procedures such as a barium enema, or seek medical assistance when experiencing pain after an interventional procedure. Several strategies have been proposed to address issues related to low health literacy ( Box 11.1 ).
- •
Caregivers should focus on increasing patient recall and understanding.
- •
Information should be organized into logical blocks, and the main message should be simplified, made specific to the patient, repeated, and summarized.
- •
Patients’ understanding should be checked by asking them to repeat information in their own words.
- •
Patient-centered interviewing skills should be employed.
- •
Medical concerns should be placed in a personal context by explaining the effect of treatment on the patient’s daily activities.
Cultural differences present unique challenges to healthcare providers, complicated by the complex interrelationships among culture, race, or ethnicity and the resulting healthcare disparities. Strategies incorporating cultural competency training have been shown to be effective in addressing cultural disparities by improving the attitudes and skills of healthcare workers. Engebretson et al. proposed a practice model integrating levels of cultural competency with components of evidence-based care in an effort to make cultural competence relevant to clinical practice. Educating healthcare providers to be more aware of their own cultural beliefs and more responsive to the cultural beliefs of their patients can lead to a higher level of self-awareness and new beliefs that will translate to better healthcare.
Communication of difficult results presents unique challenges that are best planned for in advance. A cancer diagnosis can involve imaging examinations in which the radiologist is primarily involved and delivers bad news to patients. It has been shown that women in the United States prefer that radiologists disclose findings from mammographic imaging immediately after the examination and that radiologists be prominent contributors in treatment and prognosis. Developing resources and making them available to guide radiologists in the position of delivering difficult news are a fundamental first step. Five stages of a difficult news delivery encounter have been described ( Box 11.2 ). Potential barriers to communicating difficult news include the lack of a preexisting relationship with the patient, lack of education of physicians to deliver difficult news effectively, physician discomfort with stressful and/or emotional discussions, lack of a comfortable space to deliver the news, and variability in what actually constitutes difficult or bad news. With a bit of anticipatory preparation, all of these barriers can be mitigated to some degree.
-
Discovery : At this stage, the imaging abnormality is identified. At this time, a point person should be assigned who is able to integrate and communicate information from both the staff and family in an effective manner while focusing on the patient’s psychosocial needs. Providing a single person allows for one voice, which reduces the likelihood of conflicting information, personalizes the process and builds trust.
-
Evaluation : The patient is notified by the point person that there is a need to discuss the imaging findings. This provides a warning that something may be wrong and allows the patient a short period of time to prepare themselves for unexpected news. The point person should be updated with new information about the findings or impression and implications.
-
Alert : Escort the family to a private consult room and explain the following: “The radiologist is reviewing the images. As soon as we have more information, we want to share it with you. Let’s go to a room where the doctor can easily find you.” By now the patient has had time to mentally prepare himself or herself to receive information in a safe environment.
-
Communication : Have all contributing parties available who can participate in the conversation; the radiologist should be present no matter who has been assigned as the point person. The availability of the radiologist to answer questions or provide further detail is of tremendous value to the patient, even if unused. The disclosure should be initiated by evaluating what the patient already knows or suspects about his or her condition. This allows the point person to address the information as an extension of what the patient already knows and to clarify any points of confusion or misunderstanding.
-
Debriefing : The results are discussed with the patient and any caregivers or family. Because family members serve as an important source of emotional and social support, involving them when delivering difficult news may help the patient cope with his or her illness. When disclosing difficult news to patients, it is important to show compassion, acknowledge the patient’s grief, and promote direct, honest communication.
Physical Comfort
The dimension of physical comfort encompasses two distinct tasks relevant to radiology, controlling acute pain and minimizing the stresses of the hospital’s physical environment to provide a supportive atmosphere for healing and recovery.
Aggressive pain management is essential to patient-centered care, yet despite advances in the use of narcotics and other analgesics, pain control continues to be one of the most feared and debilitating aspects of illness and medical treatment. Studies assessing pain in various clinical settings indicate that a significant number of patients continue to experience moderate or severe pain despite treatment with analgesics, ranging from 20% to 75% of those questioned. For interventional procedures, radiologists should perform a baseline assessment by asking patients to rate their pain, make regular and ongoing assessments of pain, and monitor the effectiveness of pain control measures as well as side effects. A study measuring patient satisfaction during four diagnostic imaging procedures found that patients experienced the highest degree of pain during mammography and double-contrast barium enema examinations; the authors concluded that pain reduction strategies should be employed. General strategies that can improve pain management include educating patients about their right to pain relief, encouraging patients to take an active role in communicating and managing their pain, making pain assessment data more visible to caregivers, and educating staff about pain control protocols with a discussion of misconceptions about narcotics and their risks and benefits.
The physical environment can have a significant impact on a patient’s experience, and a supportive environment may serve to help prevent illness and alleviate stress and depression. A key factor in determining customer satisfaction with radiology services concerns tangibles , which include the physical appearance of a department, its facilities, and the quality of the equipment. According to Alderson, tangible factors have a surprisingly large impact on the patient’s opinion of a practice, because the patient’s experience of service is much broader than the core skill brought by radiologists. Examples of physical features that support a patient-centered environment include general cleanliness, availability of parking in an area that is easily accessible and well lighted, well-kept building and grounds, inviting waiting rooms, and comfortable exam rooms. The physical environment can be further individualized based on the patient population, with the Children’s Hospital of Pittsburgh being an example of patient-centered design for pediatric patients and their families. The general trend in the design of healthcare facilities is toward more private, patient-friendly environments that are clean, reduce stress, and support patient well-being.
Emotional Support
A patient’s experience of illness includes the emotional and psychological consequences of being ill, and healthcare providers must adequately address these subjective aspects of illness to provide the most effective care. Research has shown that addressing patients’ emotional needs can influence their satisfaction with care, compliance with treatment regimens, side effects from drugs, recovery of function, need for pain medications, and length of hospital stay.
Anxiety and frustration are emotions experienced by patients as a result of waiting or not knowing what to expect, especially when a procedure has the potential to elicit discomfort or pain. Anxiety is often driven or magnified by the fact that critical clinical decisions may depend on the outcome of imaging procedures, and many diagnoses (e.g., cancer) have profound physical, emotional, and psychological implications for patients and their families. Survey results from a study of women undergoing percutaneous core biopsy of the breast indicate that being concerned about the results of the biopsy was a significant contributor to patient anxiety. Approximately 50% of patients surveyed in a cancer center reported that the radiology examination worried them during the days before the appointment, with 13% of respondents reporting being considerably worried. The reasons reported were fear of the results, waiting for the results, and fear of the risks and the examination procedure.
In a study of patients undergoing interventional radiologic procedures, subjective feelings of anxiety before procedures and patient pain during procedures were assessed on a visual analog scale to evaluate the effectiveness of conscious sedation. The authors found that all patients significantly overestimated their anticipated pain and concluded that interventionalists should spend more time assessing the patient’s fear of pain and attempting to reduce that fear rather than dwelling on the technical aspects of procedures. High levels of anxiety experienced by women undergoing breast biopsy in a study evaluating correlates of anxiety led the authors to conclude that there is a need for future consideration and assessment of potential intervention strategies for anxiety. When discussing procedures with patients, it is important to give specific information with realistic expectations. Research has shown that giving patients information about the sensory aspect of procedural experiences helps reduce anxiety, whereas inaccurate expectations about the physical sensations (e.g., pain) can be a significant source of distress. Self-reporting instruments can be used to assess level of anxiety prior to procedures, and different types of educational material can be used to reduce anxiety depending on patient preference.
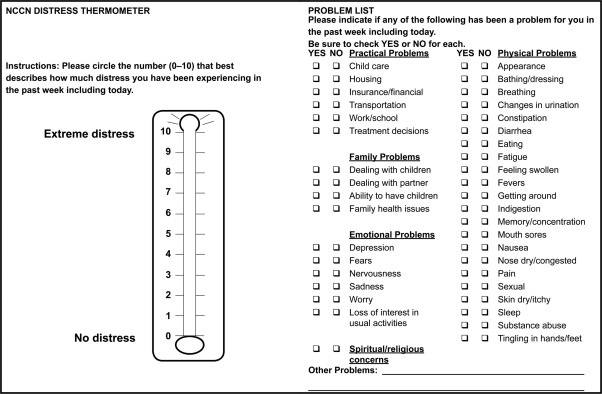
Radiologists who have relationships with patients beyond interpreting imaging examinations in the reading room should develop specific behaviors to provide emotional support for their patients that convey a genuine sense of caring and concern. According to Walker, the most important category of support for patients is the expression of positive affect or bolstering of self-esteem, which includes such actions as expressing concern and empathy, showing special understanding of the nature of the problem, calm acceptance of the problem, and the expression of optimism or hope. Beyond these general behaviors, patients differ in their needs for support, and clinicians should ask patients about their fears and anxiety, as well as what kind of emotional support they find helpful. A variety of approaches have been described to reduce stress and relieve anxiety. Sims and Rilling have described a distress tool ( Fig. 11.2 ) to evaluate and quantify patient psychosocial distress in interventional radiology patients with cancer, as well as psychosocial interventions that can be made within the interventional radiology clinic setting.
Involvement of Family and Friends
Families serve several functions in the setting of illness, including caregivers or care partners, long-term promoters of health and well-being, and providers of essential social and emotional support. Given these important roles, family involvement is an important component of patient-centered care and should be encouraged and supported. One of the most important functions of family members is to serve as proxy decision makers and patient advocates. This may put family members in an adversarial role with healthcare providers but ensures that someone is looking out for the patient’s best interests. Family members monitor the patient’s care both within the hospital setting and at home and can participate meaningfully in healthcare decisions. Radiologists can support family involvement in a patient’s care by including family members when providing information about imaging procedures or discussing abnormal findings. Including family members in the discussion of risks and benefits for imaging procedures facilitates shared decision making and is an opportunity for family members to provide information about the patient and ask questions. Family members caring for the patient at home can help ensure that patients follow postprocedural instructions, understand and identify warning signs to seek immediate care, and obtain necessary follow-up.
Methods to Assess Patient-Centeredness in Radiology
Using experiences with focus groups and patient surveys, Lexa describes four groups or clusters of issues central to how patients perceive radiology services and evaluate them: time, safety, human interactions, and creature comforts. It is important to keep in mind, however, that there is considerable variability among patients related to several factors including age, gender, culture, type of illness, magnitude of illness, and regional variability in expectations. This variability leads to inhomogeneity in patient’s definitions of subjective criteria and expectations for imaging services, emphasizing the need to assess satisfaction for patients undergoing imaging examinations at your particular facility. Box 11.3 provides a list of objective and subjective criteria that can be used to evaluate patient satisfaction with imaging service and quality using a rating scale ranging from very dissatisfied to very satisfied (e.g., Likert scale, 1 to 5). Patient satisfaction surveys can be developed to gather qualitative feedback and suggestions from patients, obtain benchmarking and comparative data, determine baseline measurements to evaluate if progress is being made toward organizational goals, or provide continual measurements to evaluate the impact of service and quality initiatives.
Time
- 1.
Appointment availability for outpatient examinations
- 2.
Appointment time for inpatient examinations
- 3.
Wait time (time from the patient arriving at the imaging facility to examination completion)
- 4.
Registration time (time to complete the registration process)
- 5.
Study time (time from the beginning of the examination to completion)
- 6.
Wait time (time from the patient arriving at the imaging facility to examination completion)
- 7.
Report turnaround time (time from examination completion to final report available for the patient or referring physician to review)
- 8.
Communication of critical results (time from examination completion to communication of critical results to the patient or referring physician)
Safety
- 1.
Perceived safety of the imaging examination
- 2.
Use of a screening tool for intravenous contrast
- 3.
Use of a screening tool for magnetic resonance imaging
- 4.
Verification of patient identity using two patient identifiers
- 5.
Verification of imaging examination to be performed
- 6.
Verification of the region or body part to be imaged
Human Interactions
- 1.
Courtesy and respectfulness of the scheduling and registration staff
- 2.
Courtesy and respectfulness of the nurses or technologists
- 3.
Courtesy and respectfulness of transport personnel
- 4.
Explanation of preparation for an imaging examination
- 5.
Explanation of what to expect during an imaging examination
- 6.
Availability of educational material about an imaging examination
- 7.
Explanation of the billing process and policies
- 8.
Availability of staff members to answer questions
Comforts
- 1.
Quality of the imaging equipment
- 2.
Parking availability and cost
- 3.
Cleanliness and accessibility of the imaging facilities
- 4.
Overall appearance of the imaging facility
Overall
- 1.
Overall satisfaction
Next Generation of Assessing Patient-Centeredness in Radiology
We have described a conceptual framework using dimensions of patient-centered care to help us understand the patient’s experience of illness and healthcare adapted to radiology. The next step in using this information to redesign radiology-specific processes and measure progress toward goals is to convert the conceptual framework into a conceptual map describing the range of experiences during the delivery of imaging and image-guided services that matter to patients. A conceptual map helps answer questions about which aspects of care matter and why, how well these are reflected in survey instruments and other assessment tools, how they could and should be valued, and how information about them should inform service development. Various conceptual and theoretical frameworks have been described including the World Health Organization’s responsiveness framework, the Institute of Medicine’s domains of healthcare quality, and Nolan et al.’s SENSES framework. The conceptual map developed by Entwistle et al. is an example of a conceptual map providing a rich array of experiences that can be used to assess patient centeredness, including healthcare relationships and their implications for people’s valued capabilities.
Patient-Centered and Patient-Defined Outcomes in Imaging
Within radiology, patient-centered outcomes are much more complex to determine and measure than patient satisfaction. A recent systematic review of the use of patient-centered outcome measures in radiology revealed only 10 publications in which the primary aim of the study was to investigate patient-centered outcomes, and none of the outcome measures used were developed specifically for radiology. The authors indicated little patient engagement in outcome research in radiology, citing barriers such as radiology departments’ research tradition, funding, and support for outcome research, coupled with the nature of the relationship between clinicians and radiology. The Patient-Centered Outcomes Research Institute is a nonprofit organization that funds comparative effectiveness research with the goal of determining which healthcare options will work best for patients in specific circumstances and then promoting policy change to promote those interests. A review of opportunities for patient-centered outcomes research in radiology was recently published.
Patient-Centered Care Competencies and Teaching Patient-Centered Skills
The American College of Graduate Medical Education (ACGME) has transitioned to an outcomes-based milestones framework for determining resident and fellow performance within six core competencies including patient care and interpersonal skills and communication. This framework allows for the assessment of the development of resident and fellow physicians in key dimensions of the elements of physician competency in radiology. The milestone addressing interpersonal and communication skills tracks the development of effective communication with patients, families, and caregivers over five subcompetencies including communicating information about imaging results, obtaining informed consent, and communicating difficult news, performing each in a compassionate and sensitive manner that adapts to the wide range of cultural, language, impairment, and health literacy differences that exist among patients. The requirement for demonstration of “interpersonal and communication skills that result in the effective exchange of information and collaboration with patients, their families, and health professionals” requires a patient-centered approach that should be developed during residency.
Developing these interpersonal and communication skills during radiology residency is challenging because the opportunities may be relatively infrequent, particularly in circumstances where diagnostic errors, procedural complications, and bad news need to be communicated. To more effectively develop proficiency, manage the stress associated with these circumstances, and further develop this core competency, the Program to Enhance Relational and Communication Skills has developed an experiential workshop. Radiology residents and other healthcare professionals learn to address difficult situations by practicing each scenario with actors trained in improvisation. The result was a significant increase in comfort with discussing radiation risks, delivering difficult diagnostic news, and communicating about medical errors. There are various templates available in the literature to help promote patient-centered communication and assist radiology trainees and radiologists alike with the disclosure of emotional or distressing results.
Conclusion
Effective delivery of care in a modern healthcare environment requires that patients be the central focus of our efforts. Although we have discussed the core considerations of this approach, opportunities to expand on these principles in radiology are vast and only partially explored here. We noted that clear benefits in patient outcomes have been demonstrated when patient care is redesigned to accommodate patient differences, address socioeconomic and cultural barriers, engage patients in their care, and anticipate patient needs. Each dimension of patient-centered care discussed here (patient values, preferences, and needs, coordination of care, communication and education, physical comfort, emotional support, and involvement of family and friends) serves as a guide to help focus future improvement efforts. Moreover, the changing healthcare landscape requires that radiologists define and measure the value of services provided, in which patient centeredness is essential. To demonstrate value, current assessment tools for patient centeredness will require a new framework to help us understand the patient’s experience of illness and healthcare. Using this framework, radiology practices can be redesigned to better align with patients’ needs and values. This approach will allow us to overcome the challenges facing radiology today and play a meaningful role in shaping the future of the specialty.
Suggested Readings
- ACGME Program Requirements for Graduate Medical Education in Diagnostic Radiology: ACGME. < https://www.acgme.org/Portals/0/PDFs/Milestones/DiagnosticRadiologyMilestones.pdf >.
- Alderson P.O.: Customer service and satisfaction in radiology. AJR Am J Roentgenol 2000; 175: pp. 319-323.
- Baile W.F., Buckman R., Lenzi R., Glober G., Beale E.A., Kudelka A.P.: SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000; 5: pp. 302-311.
- Baker D.W., Hayes R., Fortier J.P.: Interpreter use and satisfaction with interpersonal aspects of care for Spanish-speaking patients. Med Care 1998; 36: pp. 1461-1470.
- Baker D.W., Parker R.M., Williams M.V., Coates W.C., Pitkin K.: Use and effectiveness of interpreters in an emergency department. J Am Med Assoc 1996; 275: pp. 783-788.
- Barry M.J., Fowler F.J., Mulley A.G., Henderson J.V., Wennberg J.E.: Patient reactions to a program designed to facilitate patient participation in treatment decisions for benign prostatic hyperplasia. Med Care 1995; 33: pp. 771-782.
- Bazzocchi M.: Doctor-patient communication in radiology: a great opportunity for future radiology. Radiol Med 2012; 117: pp. 339-353.
- Beach M, Cooper L, Robinson K, et al. Strategies for improving minority healthcare quality Baltimore: agency for healthcare research and quality. < https://archive.ahrq.gov/downloads/pub/evidence/pdf/minqual/minqual.pdf >.
- Berkman N.D., Sheridan S.L., Donahue K.E., Halpern D.J., Crotty K.: Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011; 155: pp. 97-107.
- Berlin L.: Communicating results of all outpatient radiologic examinations directly to patients: the time has come. AJR Am J Roentgenol 2009; 192: pp. 571-573.
- Bohachick P.: Progressive relaxation training in cardiac rehabilitation: effect on psychologic variables. Nurs Res 1984; 33: pp. 283-287.
- Brock D.W.: The ideal of shared decision making between physicians and patients. Kennedy Inst Ethics J 1991; 1: pp. 28-47.
- Brown S.D., Callahan M.J., Browning D.M., et. al.: Radiology trainees’ comfort with difficult conversations and attitudes about error disclosure: effect of a communication skills workshop. J Am Coll Radiol 2014; 11: pp. 781-787.
- Carey M.P., Burish T.G.: Providing relaxation training to cancer chemotherapy patients: a comparison of three delivery techniques. J Consult Clin Psychol 1987; 55: pp. 732-737.
- Carrasquillo O., Orav E.J., Brennan T.A., Burstin H.R.: Impact of language barriers on patient satisfaction in an emergency department. J Gen Intern Med 1999; 14: pp. 82-87.
- Charles C., Gafni A., Whelan T.: Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med 1999; 49: pp. 651-661.
- Cincinnati Children’s Hospital Medical Center. Communicating Difficult News to Patients and Families. < http://cchmcstream.cchmc.org/MediasiteEX/Play/352006b8b86c44378c1f0bb9dca868301d >.
- Cobb S.C.: Teaching relaxation techniques to cancer patients. Cancer Nurs 1984; 7: pp. 157-161.
- Cohen F.L.: Postsurgical pain relief: patients’ status and nurses’ medication choices. Pain 1980; 9: pp. 265-274.
- Cohen M.D., Alam K.: Radiology clinical synopsis: a simple solution for obtaining an adequate clinical history for the accurate reporting of imaging studies on patients in intensive care units. Pediatr Radiol 2005; 35: pp. 918-922.
- Cotanch P.H., Strom S.: Progressive muscle relaxation as antiemetic therapy for cancer patients. Oncol Nurs Forum 1987; 14: pp. 33-37.
- Crane J.A.: Patient comprehension of doctor-patient communication on discharge from the emergency department. J Emerg Med 1997; 15: pp. 1-7.
- Deber R.B., Kraetschmer N., Irvine J.: What role do patients wish to play in treatment decision making?. Arch Intern Med 1996; 156: pp. 1414-1420.
- Devine E.C., Cook T.D.: A meta-analytic analysis of effects of psychoeducational interventions on length of postsurgical hospital stay. Nurs Res 1983; 32: pp. 267-274.
- Emanuel E.J., Emanuel L.L.: Four models of the physician-patient relationship. J Am Med Assoc 1992; 267: pp. 2221-2226.
- Engebretson J., Mahoney J., Carlson E.D.: Cultural competence in the era of evidence-based practice. J Prof Nurs 2008; 24: pp. 172-178.
- Entwistle V., Firnigl D., Ryan M., Francis J., Kinghorn P.: Which experiences of health care delivery matter to service users and why? A critical interpretive synthesis and conceptual map. J Health Serv Res Policy 2012; 17: pp. 70-78.
- Fagan M.J., Diaz J.A., Reinert S.E., Sciamanna C.N., Fagan D.M.: Impact of interpretation method on clinic visit length. J Gen Intern Med 2003; 18: pp. 634-638.
- Fast Company. Patient Centered Design: children’s Hospital of Pittsburgh. < https://www.fastcompany.com/1351198/patient-centered-design-childrens-hospital-pittsburgh >.
- Flores G., Laws M.B., Mayo S.J., et. al.: Errors in medical interpretation and their potential clinical consequences in pediatric encounters. Pediatrics 2003; 111: pp. 6-14.
- Gandhi T.K., Burstin H.R., Cook E.F., et. al.: Drug complications in outpatients. J Gen Intern Med 2000; 15: pp. 149-154.
- Gerteis M.: Picker/Commonwealth Program for Patient-Centered Care. Through the Patient’s Eyes: Understanding and Promoting Patient-Centered Care. 1993. Jossey-Bass San Francisco
- Gunderman R.B., Brown B.P.: Teaching interpersonal and communication skills. Acad Radiol 2012; 19: pp. 1589-1590.
- Hammond I., Franche R.L., Black D.M., Gaudette S.: The radiologist and the patient: breaking bad news. Can Assoc Radiol J 1999; 50: pp. 233-234.
- Hoe J.W.: Service delivery and service quality in radiology. J Am Coll Radiol 2007; 4: pp. 643-651.
- Iezzoni L.I., O’Day B.L., Killeen M., Harker H.: Communicating about health care: observations from persons who are deaf or hard of hearing. Ann Intern Med 2004; 140: pp. 356-362.
- Institute of Medicine (US) : Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system for the 21st century. 2001. National Academy Press Washington, DC pp. 337p.
- Itri J.N.: Patient-centered radiology. Radiographics 2015; 35: pp. 1835-1846.
- Jacobs E., Agger-Gupta N., Chen A., Piotrowski A., Hardt E.: Language Barriers in Health Care Setting: an Annotated Bibliography of the Research Literature. 2003. The California Endowment Woodland Hills, CA
- Johnson J.E., Christman N.J., Stitt C.: Personal control interventions: short- and long-term effects on surgical patients. Res Nurs Health 1985; 8: pp. 131-145.
- Johnson J.E., Leventhal H.: Effects of accurate expectations and behavioral instructions on reactions during a noxious medical examination. J Pers Soc Psychol 1974; 29: pp. 710-718.
- Johnson J.E., Rice V.H., Fuller S.S., Endress M.P.: Sensory information, instruction in a coping strategy, and recovery from surgery. Res Nurs Health 1978; 1: pp. 4-17.
- Ka’opua L.S., Park S.H., Ward M.E., Braun K.L.: Testing the feasibility of a culturally tailored breast cancer screening intervention with Native Hawaiian women in rural churches. Health Soc Work 2011; 36: pp. 55-65.
- Karliner L.S., Jacobs E.A., Chen A.H., Mutha S.: Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007; 42: pp. 727-754.
- Karliner L.S., Kerlikowske K.: Ethnic disparities in breast cancer. Womens Health (Lond Engl) 2007; 3: pp. 679-688.
- Keeri-Szanto M., Heaman S.: Postoperative demand analgesia. Surg Gynecol Obstet 1972; 134: pp. 647-651.
- Kim J.H., Menon U., Wang E., Szalacha L.: Assess the effects of culturally relevant intervention on breast cancer knowledge, beliefs, and mammography use among Korean American women. J Immigr Minor Health 2010; 12: pp. 586-597.
- Lawlis G.F., Selby D., Hinnant D., McCoy C.E.: Reduction of postoperative pain parameters by presurgical relaxation instructions for spinal pain patients. Spine (Phila PA 1976) 1985; 10: pp. 649-651.
- Lexa F.J., Berlin J.W.: The architecture of smart surveys: core issues in why and how to collect patient and referring physician satisfaction data. J Am Coll Radiol 2009; 6: pp. 106-111.
- Lexa F.J.: 300,000,000 customers: patient perspectives on service and quality. J Am Coll Radiol 2006; 3: pp. 346-350.
- Liu S., Bassett L.W., Sayre J.: Women’s attitudes about receiving mammographic results directly from radiologists. Radiology 1994; 193: pp. 783-786.
- Loy C.T., Irwig L.: Accuracy of diagnostic tests read with and without clinical information: a systematic review. J Am Med Assoc 2004; 292: pp. 1602-1609.
- Mansell D., Poses R.M., Kazis L., Duefield C.A.: Clinical factors that influence patients’ desire for participation in decisions about illness. Arch Intern Med 2000; 160: pp. 2991-2996.
- Manson A.: Language concordance as a determinant of patient compliance and emergency room use in patients with asthma. Med Care 1988; 26: pp. 1119-1128.
- Marks R.M., Sachar E.J.: Undertreatment of medical inpatients with narcotic analgesics. Ann Intern Med 1973; 78: pp. 173-181.
- Mathers S.A., Chesson R.A., Proctor J.M., McKenzie G.A., Robertson E.: The use of patient-centered outcome measures in radiology: a systematic review. Acad Radiol 2006; 13: pp. 1394-1404.
- McNeil B.J., Weichselbaum R., Pauker S.G.: Speech and survival: tradeoffs between quality and quantity of life in laryngeal cancer. N Engl J Med 1981; 305: pp. 982-987.
- Mueller P.R., Biswal S., Halpern E.F., Kaufman J.A., Lee M.J.: Interventional radiologic procedures: patient anxiety, perception of pain, understanding of procedure, and satisfaction with medication—a prospective study. Radiology 2000; 215: pp. 684-688.
- Mumford E., Schlesinger H.J., Glass G.V.: The effect of psychological intervention on recovery from surgery and heart attacks: an analysis of the literature. Am J Public Health 1982; 72: pp. 141-151.
- Niazkhani Z., Pirnejad H., Berg M., Aarts J.: The impact of computerized provider order entry systems on inpatient clinical workflow: a literature review. J Am Med Inform Assoc 2009; 16: pp. 539-549.
- Novy D.M., Price M., Huynh P.T., Schuetz A.: Percutaneous core biopsy of the breast: correlates of anxiety. Acad Radiol 2001; 8: pp. 467-472.
- Ollivier L., Apiou F., Leclere J., et. al.: Patient experiences and preferences: development of practice guidelines in a cancer imaging department. Cancer Imaging 2009; 9: pp. S92-S97.
- Ollivier L., Leclere J., Dolbeault S., Neuenschwander S.: Doctor-patient relationship in oncologic radiology. Cancer Imaging 2005; 5: pp. S83-S88.
- Prabhakar A.M., Harvey H.B., Platt J.T., Brink J.A., Oklu R.: Engaging our patients: shared decision making and interventional radiology. Radiology 2014; 272: pp. 9-11.
- Puntillo K.A.: Pain experiences of intensive care unit patients. Heart Lung 1990; 19: pp. 526-533.
- Radner G.: It’s Always Something. 20th Anniversary Ed. 2009. Simon & Schuster New York, NY
- Revicki D.A., Yabroff K.R., Shikiar R.: Outcomes research in radiologic imaging: identification of barriers and potential solutions. Acad Radiol 1999; 6: pp. S20-S28.
- Reynolds A.: Patient-centered care. Radiol Technol 2009; 81: pp. 133-147.
- Robinson J.C.: The end of managed care. J Am Med Assoc 2001; 285: pp. 2622-2628.
- Roter D.L., Rudd R.E., Comings J.: Patient literacy. A barrier to quality of care. J Gen Intern Med 1998; 13: pp. 850-851.
- Schreiber M.H., Leonard M., Rieniets C.Y.: Disclosure of imaging findings to patients directly by radiologists: survey of patients’ preferences. AJR Am J Roentgenol 1995; 165: pp. 467-469.
- Shams-Avari P.: Linguistic and cultural competency. Radiol Technol 2005; 76: pp. 437-445.
- Sims M.J., Rilling W.S.: Psychosocial management of distress in interventional radiology patients with cancer. Tech Vasc Interv Radiol 2006; 9: pp. 101-105.
- Stacey D., Legare F., Col N.F., et. al.: Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2014; 1: CD001431
- Strull W.M., Lo B., Charles G.: Do patients want to participate in medical decision making?. J Am Med Assoc 1984; 252: pp. 2990-2994.
- US Health and Human Services. What Is Cultural Competency? < https://www.cdc.gov/nchhstp/socialdeterminants/docs/what_is_cultural_competency.pdf >.
- US National Library of Medicine, National Institutes of Health. Health Literacy. < http://www.nlm.nih.gov.easyaccess1.lib.cuhk.edu.hk/medlineplus/healthliteracy.html >.
- Van den Bergh K.A., Essink-Bot M.L., Bunge E.M., et. al.: Impact of computed tomography screening for lung cancer on participants in a randomized controlled trial (NELSON trial). Cancer 2008; 113: pp. 396-404.
- Vranceanu A.M., Cooper C., Ring D.: Integrating patient values into evidence-based practice: effective communication for shared decision-making. Hand Clin 2009; 25: pp. 83-96. vii
- Vydareny K.H., Amis E.S., Becker G.J., et. al.: Diagnostic radiology milestones. J Grad Med Educ 2013; 5: pp. 74-78.
- Waitzkin H.: Information giving in medical care. J Health Soc Behav 1985; 26: pp. 81-101.
- Weis O.F., Sriwatanakul K., Alloza J.L., Weintraub M., Lasagna L.: Attitudes of patients, housestaff, and nurses toward postoperative analgesic care. Anesth Analg 1983; 62: pp. 70-74.
- Wikipedia. Soft Skills. < http://en.wikipedia.org/wiki/Soft_skills >.
- Winkel G.H., Holahan C.J.: The environmental psychology of the hospital: is the cure worse than the illness?. Prev Hum Serv 1985; pp. 11-33.
- Zygmont M.E., Lam D.L., Nowitzki K.M., et. al.: Opportunities for patient-centered outcomes research in radiology. Acad Radiol 2016; 23: pp. 8-17.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


