Abstract
The purpose of this study is to present the indications, rationale and techniques used in minimally invasive percutaneous biopsy of the bowel. Both efficacy and rate of complications were evaluated. A series of 63 patients over a ten-year period were retrospectively reviewed. Techniques using fluoroscopy, ultrasound and CT guidance are described.
Percutaneous biopsy of the bowel is a safe and effective method for obtaining histological samples in selected patients who are not fit for endoscopy or for other technical reasons. Radiologists should be aware of its potential as a valid alternative.
1
Introduction
The standard process for obtaining histological samples from intestinal lesions is through endoscopy, push enteroscopy or colonoscopy. In certain instances samples may be obtained via laparotomy when access through endoscopic techniques is unachievable. The indications for percutaneous biopsy of the small or large bowel are less common. Percutaneous image guided biopsies may be required if endoscopic sampling is difficult or inadequate. Patients who are unfit for surgery or with contraindications to general anaesthesia may require the less invasive percutaneous approach. In certain palliative cases where chemotherapy is being envisaged a minimally invasive histological sampling may be preferred. Other indications include recurrent known pathology, for example, lymphoma of the bowel, where patients are unwilling to undergo laparotomy for histological samples and in patients in whom in percutaneous biopsy may be considered safer than an operative procedure due to haematological or bleeding disorders. Finally, the lack of accessible distant metastases for biopsy (such as in the liver) may be an indication of minimally invasive percutaneous biopsy of relatively inaccessible lesions.
In this case series and technical review, techniques for obtaining percutaneous biopsies using fluoroscopy, ultrasound, and CT guidance are described. A review of a large series of 63 patients has been described, with guidance based on learning experience of the operators.
2
Materials and methods
A retrospective review of patient records was performed between January 2011–November 2022 (limited cases during COVID pandemic between 2019 and 2021) and 63 patients were identified who underwent image guided percutaneous biopsy of the small or large bowel. Histological results were evaluated to determine adequacy of sampling. Post biopsy clinical notes were scrutinized to assess for post biopsy complications or adverse outcomes.
3
Results
Four patients underwent FNAC and the remaining 59 patients had core biopsies. 13 patients had recurrent bowel lesions and histology was needed for further treatment and molecular analysis. The other 50 cases underwent percutaneous biopsies due to a combination of frailty, anaesthetic contraindications, haematological contraindications for surgery and prior inadequate results. Three of the four patients who underwent FNAC had positive cytology samples (75 %). 51 patients had adequate histological samples from core biopsies (86.4 %). In 8 patients adequate samples could not be obtained or the procedure was abandoned due to technical difficulty in obtaining safe biopsy. Two patients who had core biopsies had small pneumoperitoneum that resolved spontaneously (3.4 %). One patient had a localized abscess at site of biopsy that resolved with antibiotics. None of the patients who had FNAC developed abscess or pneumoperitoneum. All FNAC procedures were carried out under ultrasound guidance. A total of 38 patients had ultrasound guided core biopsies; 3 patients had fluoroscopic guided procedures; and 18 patients had CT guided biopsies.
4
Discussion and technical review
Each imaging modality and biopsy equipment provides its own advantages during biopsy of intestinal lesions. Biopsy samples can be obtained via Fine Needle Aspiration Cytology (FNAC) or Cutting Core Needle Biopsy. Core biopsies are generally considered to be superior to FNAC as tissue architecture is better preserved for histological assessment [ ]. In this series an 18- or 20-gauge cutting needle was used for bowel samples. Biopsy attempts were made ensuring that the lumen was not traversed wherever possible. Although traversing the lumen of the bowel was avoided, previous large series of the percutaneous pancreatic biopsies through the gastric wall have not reported any significant complications related to breach of the stomach wall [ , ]. Similarly, in our experience, transluminal biopsy of the small bowel with needles of 18-gauge or smaller did not cause significant complications. If a FNAC procedure is planned, it is useful to have a cytologist on hand to review samples to obviate the need for multiple needle passes and assess adequacy [ ].
4.1
Fluoroscopic guided biopsy
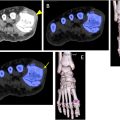
Fluoroscopic guided biopsies of the intestine are rarely performed and in this series there were only 3 such cases (4.76 %). Fluoroscopic guidance for biopsies may be indicated in cases where ultrasound or CT guidance for percutaneous approach is technically difficult or challenging such as areas under the ribcage, access which requires a steeply angled approach or where real-time imaging is advantageous. Fluoroscopic guidance has been shown to be an effective procedure with few major complications [ ]. Advantages of fluoroscopy is its temporal resolution-where needle placement within a lesion can be done in dynamic, real time [ ]. With this method, the authors find it helpful to opacify the bowel with enteral contrast such as barium or gastrografin. Outlining of the bowel allows accurate delineation of the abnormal area for targeted biopsy [ Figs. 1–2 ]. Identification of the abnormal area also allows the operator to apply manual abdominal compression to stabilise the lesion for biopsy or displace overlying structures [ Figs. 3–4 ].




Related posts:
 Assessing the reliability of ChatGPT4 in the appropriateness of radiology referrals
Assessing the reliability of ChatGPT4 in the appropriateness of radiology referrals
 Treatment of follicular lymphoma with a focus on radiotherapy
Treatment of follicular lymphoma with a focus on radiotherapy
 Dual energy CT for the diagnosis of gout: Evaluating the optimal Hounsfield unit setting for dual energy processing
Dual energy CT for the diagnosis of gout: Evaluating the optimal Hounsfield unit setting for dual energy processing
 Evaluating intra and inter-observer bias in the cosmetic rating for random vs. serial assessment of breast photographs
Evaluating intra and inter-observer bias in the cosmetic rating for random vs. serial assessment of breast photographs
 Determinants of aesthetic outcome after breast conserving surgery: A prospective cohort study
Determinants of aesthetic outcome after breast conserving surgery: A prospective cohort study
 Age is a risk factor for long-term effects of chemotherapy on dental development in childhood cancer survivors
Age is a risk factor for long-term effects of chemotherapy on dental development in childhood cancer survivors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


