Physics, Artifacts, NRC, Quality Control, and Safety
QUESTIONS

A. 511 keV
B. 1,022 keV
C. 511 MeV
D. 1,022 MeV
View Answer
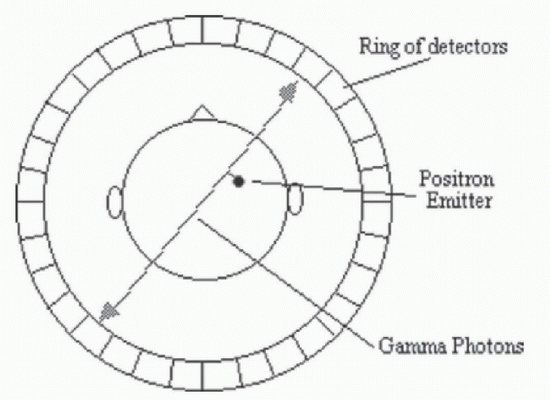
1 Answer A. An anterior maximum intensity projection (MIP) image demonstrates physiologic distribution of radiopharmaceutical within the gray matter of the brain, lymphoid and glandular tissues of the neck, myocardium, liver, and GI and GU systems. This is an F-18 FDG positron emission tomography (PET) scan. A positron emitted from the F-18 nucleus undergoes annihilation as it interacts with an electron; this annihilation event produces two 511 keV photons, which are detected by a ring of detectors surrounding the patient. Coincidence counting is used to differentiate true events from random events/noise. The diagram below demonstrates a positron annihilation event producing two 511 keV photons.
 |
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:43-48.
Saha GB. Fundamentals of nuclear pharmacy, 6th ed. New York, NY: Springer, 2010:45.
http://users.fmrib.ox.ac.uk/˜stuart/thesis/chapter_3/section3_1.html
A. Converging
B. Diverging
C. Parallel
D. Pinhole
View Answer
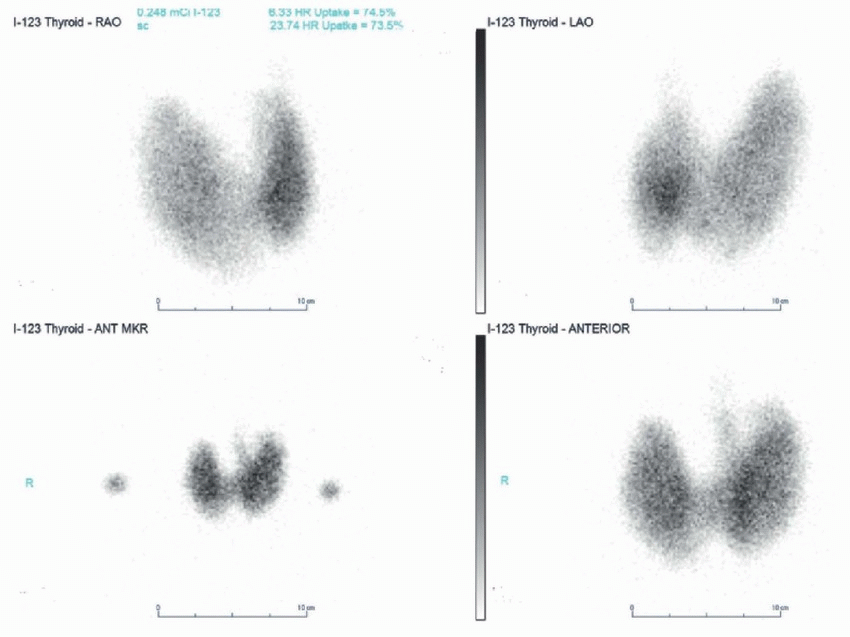
2 Answer D. Thyroid images are acquired with a pinhole collimator. Pinhole collimators are used for small organs such as thyroid. Converging collimators are used when the target organ is smaller than the size of the detector, while diverging collimators are used when the target organ is larger than the detector. Parallel collimators are used for most examinations and are considered the workhorse of the nuclear medicine department.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:29-31.
3 How would the images acquired with the gamma camera with crystal thickness of 5/8 inch compare with the gamma camera with crystal thickness of 3/8 inch?
A. Increased resolution
B. Increased sensitivity
C. Decreased interaction of gamma rays
D. Increased transmission of gamma rays
E. Decreased light production
View Answer
3 Answer B. Increasing the thickness of gamma camera crystals will result in increased sensitivity secondary to increased interaction and absorption of gamma rays, which will ultimately result in more light production. However, this will result in decreased resolution.
Reference: Saha GB. Fundamentals of nuclear pharmacy, 6th ed. New York, NY: Springer, 2010:41-42.
4 Which of the following organs would be visualized with excessive aluminum in the Tc-99m sulfur colloid kit?
A. Liver
B. Muscle
C. Heart
D. Lung
E. Brain
View Answer
4 Answer D. Excessive amounts of aluminum in the Tc-99m sulfur colloid kit results in diffuse lung uptake.
Reference: Goldfarb CR, Cooper JA, Parmett SR, et al. Nuclear medicine board review. New York, NY: Thieme, 1998:18.
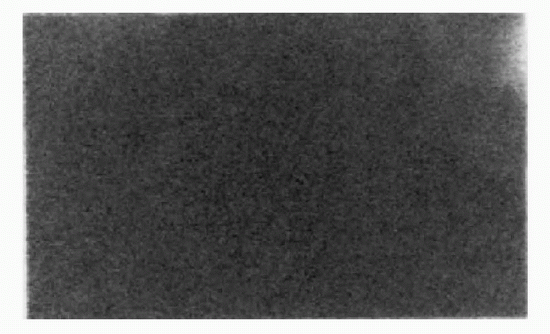
5 When reviewing the morning QC images, the technologist notes the following finding on the extrinsic flood image, which was not present on the intrinsic flood image. What is the most likely cause for this finding?
 |
A. Problem with the sealed source used to acquire flood
B. Problem with the collimator
C. Problem with the gamma camera detector
D. Problem with the software used to process data
View Answer
5 Answer B. Extrinsic floods are acquired with the collimator in place. The fact that the defect is seen with the extrinsic flood images only means that the problem resides in the collimator (i.e., cracked collimator). If the problem was with the gamma camera detector or sealed source, an abnormality would have been seen both with (extrinsic) and without (intrinsic) the collimator. Flood images could be repeated with a different source if one wants to differentiate between a problem with the detector and a problem with the source.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:55-60.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:47-48.
6 A technologist states that there is an unknown radionuclide spilled on the countertop. Which of the following devices could be utilized to identify what radionuclide was spilled?
A. Geiger-Muller counter
B. Ionization survey chamber
C. Dose calibrator
D. Well counter
View Answer
6 Answer D. Geiger-Mueller counters are very sensitive handheld instruments that are used to detect small amounts of radioactive contamination. The detector is gasfilled with high voltage applied from the anode to the cathode resulting in cascade of events from a single gamma ray. They are not energy discriminating and have high dead time, which prevents their use in high radiation areas. Ionization survey chambers are used to measure low or high exposure rates. They are filled with gas or air and have a relatively low voltage applied from anode to cathode, which means they have shorter dead times and can be used to measure high radiation exposure areas. Dose calibrators are a type of ionization chamber used to assay the amount of activity in vials/syringes from a known radiopharmaceutical. Well counters are composed of NaI crystals with a hole in them to place the sample. This results in an ability to detect very small quantities of radioactivity. However, because of the high detection efficiency and longer dead time, they cannot be used with large amounts of radioactivity. One can analyze the energy spectrum by combining the well counter with a multichannel analyzer and thus determine the specific radioisotope that may have been spilled on the countertop.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:23-25.
7 Which of the following instruments is used for performing a contamination survey?
A. Geiger-Muller counter
B. Ionization survey chamber
C. Dose calibrator
D. Well counter
View Answer
7 Answer A. Geiger-Mueller counters are very sensitive handheld instruments that are used to detect small amounts of radioactive contamination. The detector is gas-filled with high voltage applied from the anode to the cathode resulting in cascade of events from a single gamma ray. They are not energy discriminating and have high dead time, which prevents their use in high radiation areas. Geiger-Mueller detectors with pancake probes are good instruments to locate any contaminated surface. Ionization survey chambers are used to measure low or high exposure rates. They are filled with gas or air and have a relatively low voltage applied from anode to cathode resulting in shorter dead times. As such, they can be used in high radiation exposure areas. Dose calibrator is a type of ionization chamber used to assay the amount of activity in vials/syringes from a known radiopharmaceutical. Well counters are composed of NaI crystals with a hole in them to place the sample. This results in an ability to detect small quantities (i.e., wipe test).
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:23-25.
8 Which of the following quality assurance tests assesses the effect due to the volume and location of a source within the dose calibrator?
A. Accuracy
B. Constancy
C. Linearity
D. Geometry
View Answer
8 Answer D. The response of a dose calibrator is dependent on the position, size, shape, and material of the source container as well as the volume of the source. Geometry is the quality assurance test that assesses the effect due to the volume and location of the source in the dose calibrator. This test is performed at installation, after repair, after recalibration, or upon moving the instrument. Geometric efficiency is the fraction of emitted radioactivity that is incident on the detection portion of the counter.
Linearity is the ability of the calibrator to accurately measure radioactivity at all clinically applicable low to high levels.
Accuracy refers to the ability of the calibrator to accurately assay samples with all clinically applicable radionuclide energies (low, medium, and high). Accuracy is checked at installation and then annually.
Constancy measures the instrument’s precision and is intended to show the reproducibility of measurements. A long-lived source such as Cs-137 is measured daily and the measurements should be within +/−5%. Constancy is tested at installation and daily.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:56.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:13.
9 What type of quality assurance is being performed when the nuclear pharmacist assays a high activity vial of Tc-99m using calibrated lead shields to simulate lower levels of radioactivity?
A. Accuracy
B. Constancy
C. Linearity
D. Geometry
View Answer
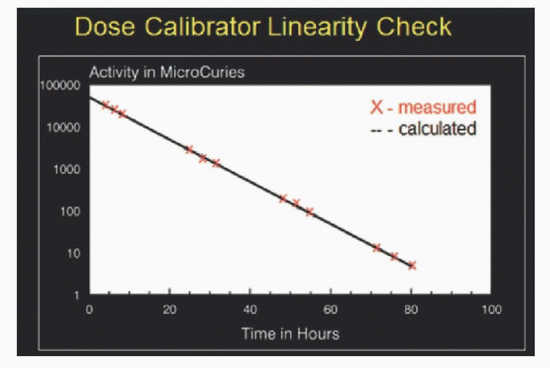
9 Answer C. The nuclear pharmacist is checking linearity. Linearity (see diagram below) is the ability of the calibrator to accurately measure radioactivity at all clinically applicable levels. This can be evaluated by one of two following methods: (1) Assay a high activity vial of Tc-99m over an 80-hour period, or (2) assay a high-activity vial of Tc-99m using calibrated lead shields to simulate lower levels of radioactivity. Linearity is checked at installation and then quarterly.
 |
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:56.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:13.
A. Geiger-Muller counter
B. Survey meter
C. Dose calibrator
D. Well counter
View Answer
10 Answer A. This is a Geiger-Muller counter with a detector probe that has pancake configuration. They can also have detector probe with a cylindrical configuration. Geiger-Mueller counters are very sensitive handheld instruments that are used to detect small amounts of radioactive contamination. The detector is gas-filled with high voltage applied from the anode to the cathode resulting in cascade of events from a single gamma ray. They are not energy discriminating and have high dead time, which prevents their use in high radiation areas.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:23-25.
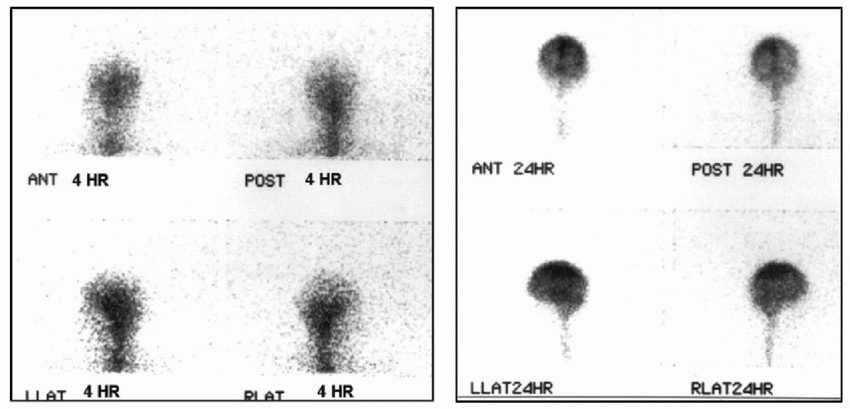
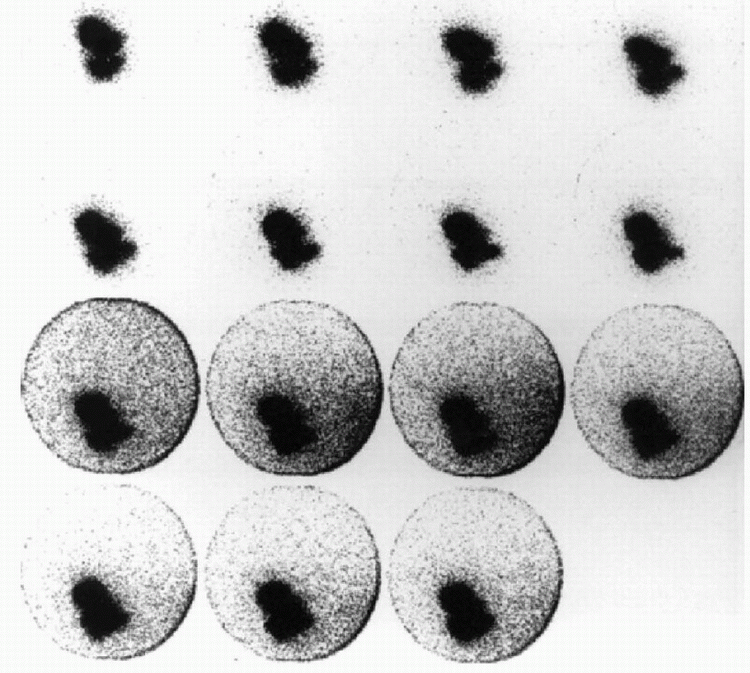
11 The following 4- and 24-hour cisternogram images were acquired after intrathecal administration of 500 µCi of In-111 DTPA. Which of the following is the most likely explanation for the image deterioration at 4 hours?
 |
A. Dose infiltration
B. Prior nuclear study
C. Change in photopeak
D. Patient scanned in adjacent room with In-111
View Answer
11 Answer C. Significantly poor image quality is present with poor count statistics on the 4-hour images. The 24-hour images demonstrate better quality and better count statistics. The findings are likely secondary to change in photopeak. The initial exam was likely acquired at a wrong photopeak with proper acquisition on the subsequent 24-hour exam. Acquisition at a wrong photopeak would result in decreased resolution and decreased sensitivity depending on the window selected and peak energy of the radiopharmaceutical. While dose infiltration would result in poor count statistics, it would appear the same on 24-hour images and would not explain better images at the 24-hour time point. Having a patient scanned in an adjacent room with a high-energy radiopharmaceutical such as F-18 FDG can cause image degradation; however, this would not occur with In-111. There is no evidence of a prior nuclear study as there is no evidence of altered biodistribution.
Reference: Habibian M, et al. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:516-521.
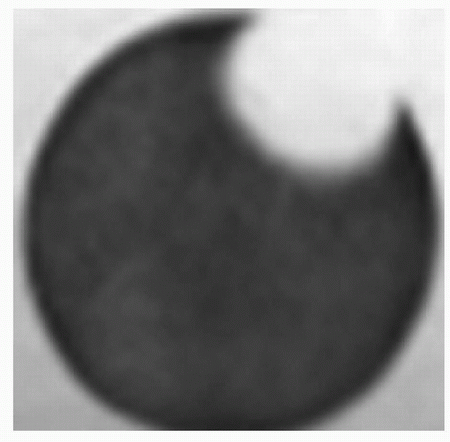
12 While performing the morning intrinsic uniformity evaluation, the technologist obtains the following image. What is the most likely etiology?
 |
A. Cracked crystal
B. Cracked collimator
C. Abnormal center of rotation
D. Nonfunctioning photomultiplier tube
View Answer
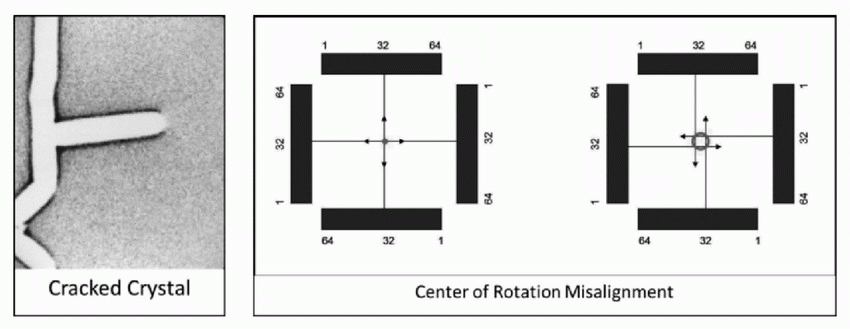
12 Answer D. The image demonstrates a peripheral crescent-shaped defect on the flood image, this is classic for a nonfunctioning photomultiplier tube. Cracked crystal (image below) would not be round in shape. Center of rotation (COR) errors are seen on SPECT images and not on planar images. The maximal uncorrected COR error allowable is 0.5 pixels. With small COR errors, a point source appears blurred, and with large COR errors, point source would appear as a doughnut (image below).
 |
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:57-61.
A. Spatial resolution
B. Energy resolution
C. Energy linearity
D. Collimator integrity
E. Uniformity
View Answer
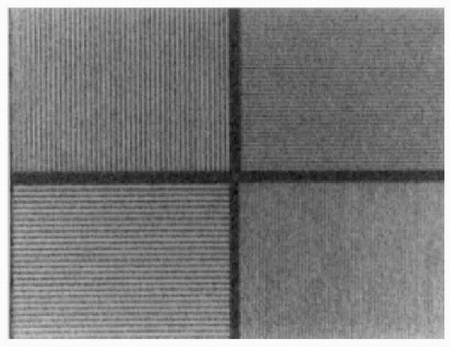
13 Answer A. Bar phantoms are used to evaluate spatial resolution and linearity on a weekly basis. The bars in each quadrant are different widths and separated by smaller differences. The ability of the system to clearly resolve the lines is representative of the resolution of the system. The phantom should be rotated 90 degrees to check the resolution in each quadrant of the camera. Linearity is tested by determining if the bars appear straight or wavy. Energy resolution is evaluated using full width at half-maximum of Tc-99m expressed as a percentage. Energy linearity is measured by testing multiple radionuclide photopeaks being within +/−5% of true value. Collimator integrity is tested by doing a high count rate flood. Uniformity is checked by doing flood images daily.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:55-56.
14 The following images are all from the same gastric emptying study with Tc-99m sulfur colloid. What is the most likely cause of the difference between the top two rows and the bottom two rows of images?
 |
A. Radiotracer decay
B. Dose infiltration
C. Free pertechnetate
D. Nearby radionuclide
View Answer
14 Answer D. The bottom row of images demonstrates significant increase in background. This is secondary to scatter from high-energy photons. In this case, a patient who had an earlier PET scan walked into the adjacent room. The half-life of Tc-99m is 6 hours; there is not enough decay over the course of the examination to cause degradation in the images. Also, the counts that are acquired are corrected to adjust for decay to ensure that gastric emptying percentages are accurate. Gastric emptying studies are performed using an oral meal; therefore, it is not possible for the dose to infiltrate. Free pertechnetate would demonstrate uptake in stomach and thyroid and would not be expected to contribute to background activity, nor would the amount of background activity be expected to change.
Reference: Habibian M, et al. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:516-521.
15 How often should the uniformity flood images be acquired?
A. Daily
B. Weekly
C. Biweekly
D. Monthly
E. Quarterly
F. Annually
View Answer
15 Answer A. Uniformity floods should be obtained daily to evaluate both the intrinsic function of the camera and the extrinsic function of the collimators. All cameras have some degree of field inhomogeneity, which can usually be corrected by performing a flood and subsequent correction. Use of a camera with an inhomogeneous field could result in misinterpretation of scan findings.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:56-57.
16 How often should the spatial resolution be tested?
A. Daily
B. Weekly
C. Biweekly
D. Monthly
E. Quarterly
F. Annually
View Answer
16 Answer B. Spatial resolution should be tested weekly. Spatial resolution refers to the ability of the system to discern discrete but contiguous sources of radioactivity. Inherent spatial resolution is the ability of the crystal, photomultiplier tube detector, and accompanying electronics to record the exact location of the light pulse on the sodium iodide crystal. Overall spatial resolution is the resolution capacity of the entire system including camera, collimator resolution, septal penetration, and scatter radiation. This can be tested with bar phantoms or with full width at half maximum.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:34-35.
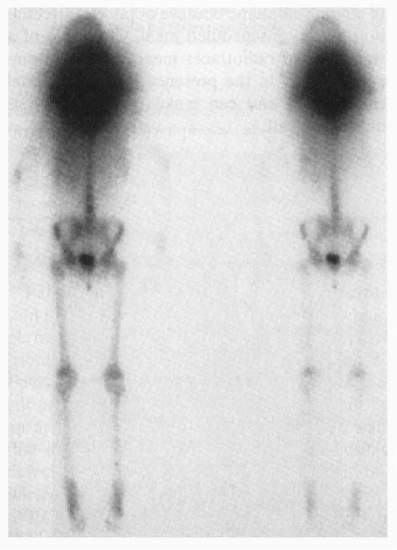
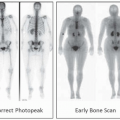
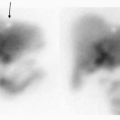
17 The following bone scintigraphy was performed to evaluate for osseous metastasis. What is the most likely explanation for the findings?
 |
A. Wrong photopeak
B. Dose infiltration
C. Thyroiditis
D. Free pertechnetate
E. Prior nuclear study
F. Photomultiplier tube malfunction
View Answer
17 Answer E. The study demonstrates intense uptake, which is ballooning out from the neck region. This degree of uptake is too intense for free Tc-99m pertechnetate. Bone scintigraphy agents do not localize in the thyroid gland and as such would not image thyroiditis. The abnormal findings on this exam are because the patient recently had radioiodine study. When a scan does not have a proper biodistribution, one should consider if there are interfering medications or if the patient has had a prior nuclear medicine examination. Having the wrong photopeak selected would result in poor resolution/count image and would not explain the intense uptake seen in the neck. Since the radiopharmaceuticals are administered by peripheral intravenous access, infiltrations in the neck would be atypical. Also, it would not explain this degree of ballooning, which in this case was secondary to marked septal penetration of low-energy collimators by the radioiodine. A malfunctioned photomultiplier tube would show up as a cold defect not a hot artifact.
References: Habibian M, et al. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:516-521.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:59.
18 What is the maximum allowable molybdenum-99 breakthrough limit in a Mo-99/Tc-99m generator eluate?
A. 0.15 µCi/mCi
B. 1.5 µCi/µCi
C. 1.5 mCi/mCi
D. 1.5 mCi/µCi
E. 1.5 µCi/mCi
View Answer
18 Answer A. The maximum allowable limit of molybdenum-99 (Mo-99) breakthrough is 0.15 µCi per 1 mCi of Tc-99m at the time of radiopharmaceutical injection. This is an example of radionuclide impurity. Excess Mo-99 leads to unnecessary increase in patient radiation dose. With time, the amount of Mo-99 breakthrough increases in a sample secondary to its longer half-life of 2.8 days. One can test for Mo-99 breakthrough by placing the eluate in a 6-mm-thick lead container to stop all 140-keV photons from Tc-99m and then counting only 740 and 780 keV photons that arise from Mo-99.
Reference: Saha GB. Fundamentals of nuclear pharmacy, 6th ed. New York, NY: Springer, 2010:77.
19 What is the maximal allowed exposure to other members of the public from a patient who has received an outpatient I-131 therapy?
A. 0.5 mSv
B. 1 mSv
C. 5 mSv
D. 10 mSv
E. 50 mSv
View Answer
19 Answer C. Under the current regulations, a patient may be released home if the authorized user physician determines that the effective dose equivalent to the maximally exposed individual (family or caregiver) does not exceed 5 mSv (0.5 rem) from a single radioisotope treatment.
The NRC believes that its current release criterion is based on sound radiation protection principles, is sufficient to protect public health and safety, results in reduced health care costs, and allows patients to be in the comfort of their homes.
Reference: NRC.gov. http://www.nrc.gov/materials/miau/med-use-toolkit/faqs-part35.html#p1
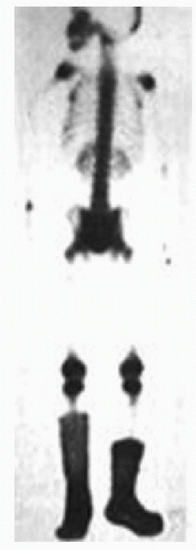
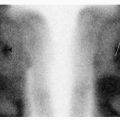
20 The following images were obtained from a pediatric bone scan. What is the most likely explanation for these findings?
 |
A. Bilateral reflex sympathetic dystrophy
B. Contamination
C. Arterial injection
D. Venous injection
E. Venous stasis
View Answer
20 Answer B. The image demonstrates intense uptake in the region of bilateral feet. Careful inspection suggests that this is not within the soft tissue or bone but is rather localized to the patient’s clothing. Specifically, it is localized within the socks bilaterally, which is often referred to as the “boot sign.” This is secondary to urine contamination. Reflex sympathetic dystrophy (RSD) is typically evaluated with a three-phase bone scan and would demonstrate increased or decreased periarticular uptake on the delayed images depending on the stage of the RSD. In the event of inadvertent arterial injections, there would be preferential increase in perfusion to a single extremity distal to the injection site. Venous stasis would result in increased activity in the soft tissues of the lower extremities; this activity is within the clothing.
Reference: Ziessman HA, Rehm P. Nuclear medicine: case review series, 2nd ed. Philadelphia, PA: Elsevier, 2011:278-280.
21 What is the dose limit to the fetus/embryo over the gestation period for a declared pregnant worker?
A. 0.5 mSv
B. 1.5 mSv
C. 5 mSv
D. 15 mSv
View Answer
21 Answer C. The dose equivalent to the embryo/fetus during the entire pregnancy from the occupational exposure of a declared pregnant woman should not exceed 5 mSv (0.5 rem). The dose equivalent to the embryo/fetus = the deep-dose equivalent to the declared pregnant woman + the dose equivalent to the embryo/fetus resulting from radionuclides in the embryo/fetus and radionuclides in the declared pregnant woman. Efforts should be made to avoid substantial variation above a uniform monthly exposure rate to a declared pregnant woman.
If the dose equivalent to the embryo/fetus is found to have exceeded 5 mSv, or is within 0.5 mSv of exceeding this dose by the time the woman declares the pregnancy to the licensee, the licensee is in compliance as long as the additional dose equivalent to the embryo/fetus does not exceed 0.5 mSv (0.05 rem) during the remainder of the pregnancy. There is no fetal dose limit if the pregnancy is not declared to the employer.
Reference: NRC.gov. http://www.nrc.gov/reading-rm/doc-collections/cfr/part020/part020-1208.html
22 What is the occupational whole body dose limit?
A. 0.5 mSv
B. 5 mSv
C. 50 mSv
D. 500 mSv
View Answer
22 Answer C. According to the NRC guidelines, the annual occupation dose limit for total effective dose equivalent is 50 mSv (5 rems).
Reference: NRC.gov.http://www.nrc.gov/reading-rm/doc-collections/cfr/part020/part020-1201.html
23 What is the occupational dose limit to the lens?
A. 0.15 mSv
B. 1.5 mSv
C. 15 mSv
D. 150 mSv
View Answer
23 Answer D. According to the NRC guidelines the annual occupation limits are as follows:
A lens dose equivalent of 150 mSv (15 rems).
The sum of the deep-dose equivalent and the committed dose equivalent to any individual organ or tissue other than the lens of the eye is 500 mSv (50 rems).
A shallow-dose equivalent of 500 mSv (50 rem) to the skin of the whole body or to the skin of any extremity.
Reference: NRC.gov. http://www.nrc.gov/reading-rm/doc-collections/cfr/part020/part020-1201.html
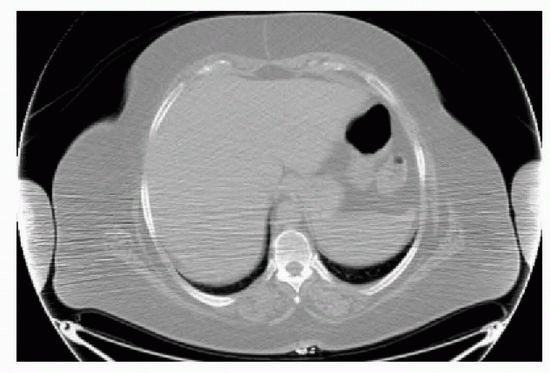
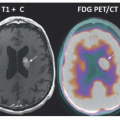
24 When reviewing the following CT images from a PET/CT scan, the technologist notices decreased quality of the images when compared to the images from a diagnostic chest CT. What is the most likely explanation for this finding?
 |
A. Beam hardening artifact
B. Contrast dose infiltration
C. FDG dose infiltration
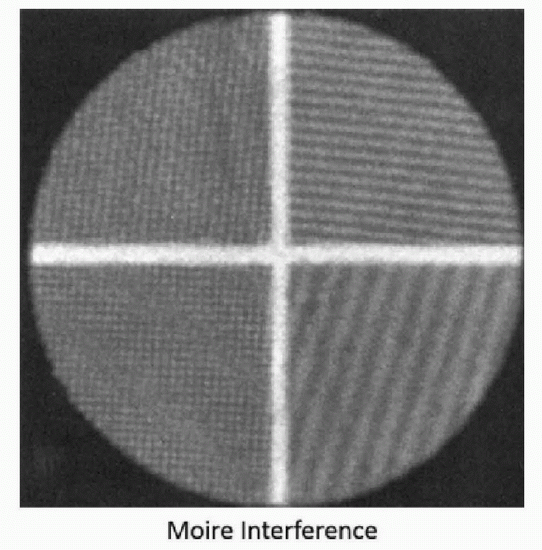
D. Moire interference
View Answer
24 Answer A. A single axial CT image demonstrates significant streak artifact from imaging with the patient’s arms down. This finding may be more pronounced on the CT acquired with PET imaging as the tube current used for attenuation correction CT scans is lower than that for the diagnostic CT. Increasing the tube current decreases this artifact but increases patient’s radiation dose. Contrast and FDG dose infiltration would not explain or cause this artifact; however, FDG dose infiltration can cause artifacts on the PET images secondary to intense activity localized at the injection site. Moire interference (shown below) is represented by wavy appearance of the images.
 |
References: Bushberg JT, et al. The essential physics of medical imaging, 2nd ed. Philadelphia, PA: LWW, 2002:369-371.
http://www.displaymate.com/moire.html
Lee MJ, Kim S, Lee SA, et al. Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics 2007;27(2):791-803.
25 What is the annual institutional limit for the amount of radioactivity that can be disposed of in the “hot sink”?
A. 1 Ci.
B. 10 Ci.
C. 100 Ci.
D. No limit.
E. One cannot purposefully dispose radioactive waste down a sink.
View Answer
25 Answer A. One sink in each laboratory may be designated as a “hot sink.” This is the only permissible location for disposing of radioactive liquid waste in the department. A log book should be set up so that each liquid waste disposal is documented by the radioisotope, amount, date, and the initials of people involved. The usual limit for the hospitals is 1 Curie per year (all radioisotopes) for all liquid waste for the entire institution. Excreta from individuals undergoing medical diagnosis or therapy with radioactive material are not subject to these limitations.
Reference: NRC.gov. http://www.nrc.gov/reading-rm/doc-collections/cfr/part020/part020-2003.html
26 After performing a liquid I-131 treatment, a resident physician notices that there is some fluid on the floor. The technologist checks the floor and everyone’s shoes and finds that there is contamination on both. How long should the contaminated material stored in isolation prior to further use?
A. 8 hours
B. 8 days
C. 30 days
D. 60 days
E. 80 days
F. 120 days
G. 160 days
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


