GROSS ANATOMY
Prostate
- •
Walnut-sized gland beneath bladder and in front of rectum
- ○
Normal prostate in young male ~ 3-cm length x 4-cm width x 2-cm depth
- ○
- •
Inverted conical shape
- ○
Base : Superior portion, continuous with bladder neck
- ○
Apex : Inferior portion, continuous with striated urinary sphincter
- ○
- •
Main function is to add nutritional secretions to sperm to form semen during ejaculation
- •
Also plays role in controlling flow of urine; prostate muscle fibers are under control of involuntary nervous system and contract to slow and stop urine
- •
Urethra traverses prostate
- ○
Verumontanum midway between base and apex where urethra makes ~ 35° bend anteriorly
- –
Openings of prostatic utricle and ejaculatory ducts
- –
Divides prostatic urethra into proximal (preprostatic) and distal (prostatic) segments
- –
- ○
Urethral crest : Narrow longitudinal ridge on posterior wall with small openings draining prostatic ducts
- ○
- •
Neurovascular bundles
- ○
Lie posterolaterally to prostate at 5- and 7-o’clock positions
- ○
Carry nerves and vascular supply to corpora cavernosa of penis (necessary for normal erection)
- ○
- •
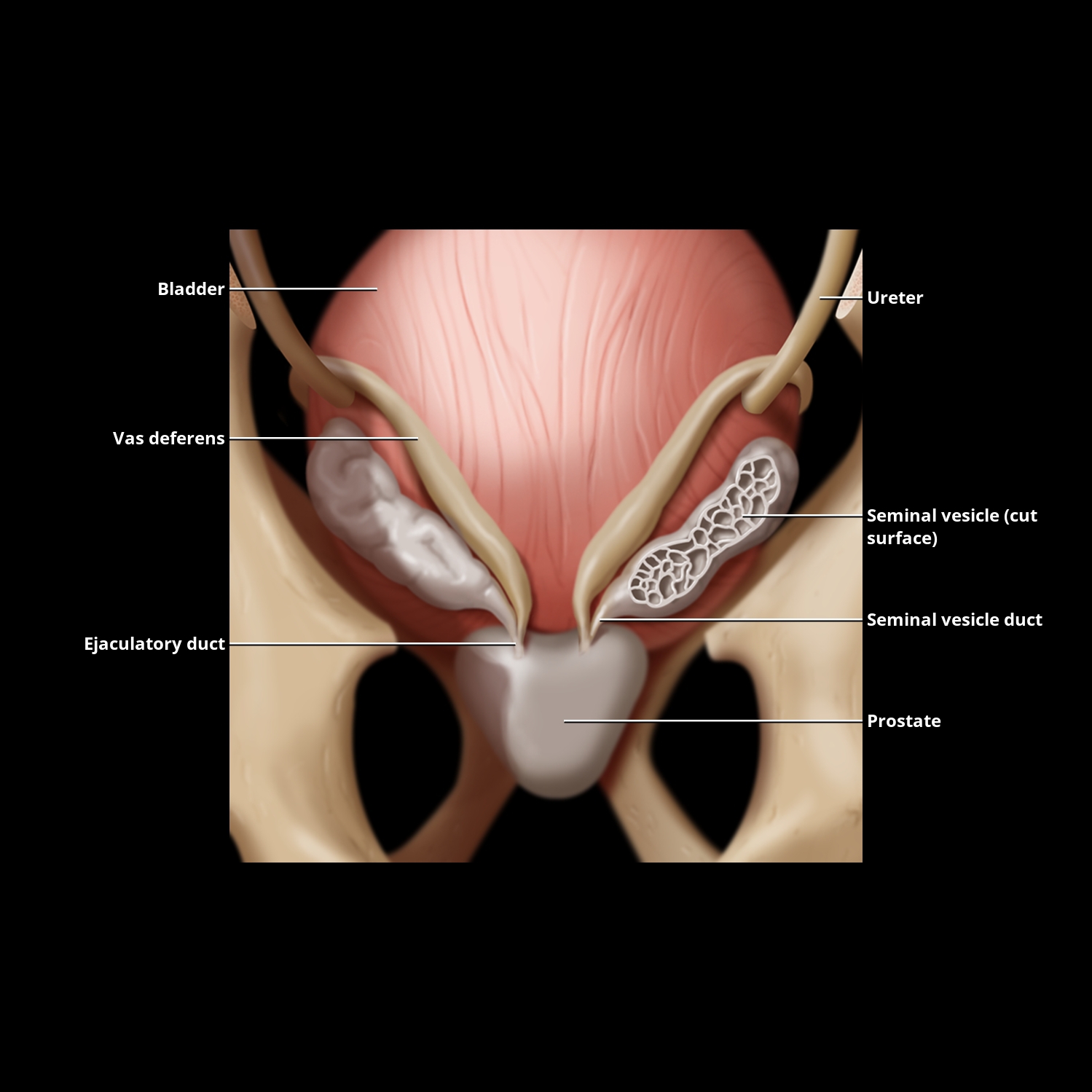
Seminal vesicles
- ○
Sac-like structures superolateral to prostate
- ○
Secrete fructose-rich fluid (energy source for sperm)
- ○
- •
Ejaculatory ducts located on either side of midline
- ○
Formed by union of seminal vesicle duct and vas deferens
- ○
Start at base of prostate and run forward and downward through gland to verumontanum
- ○
Zonal Anatomy
- •
Prostate is histologically composed of ~ 70% glandular and 30% nonglandular elements
- •
Central zone (CZ) : ~ 25% glandular tissue; cone-shaped zone around ejaculatory ducts with widest portion making majority of prostatic base
- •
Peripheral zone (PZ) : ~ 70% glandular tissue, covers posterolateral aspects of gland
- ○
Surrounds CZ and distal prostatic urethra
- ○
Zone where cancer most commonly occurs
- ○
- •
Transition zone (TZ) : 2 separate lobules surround urethra proximal to verumontanum
- ○
~ 5-10% glandular tissue in young males; can be very large in older males with benign prostatic hypertrophy (BPH)
- ○
- •
Anterior fibromuscular stroma is nonglandular tissue
- ○
Runs anteriorly from bladder neck to striated urinary sphincter
- ○
- •
Prostate pseudocapsule (“surgical capsule”)
- ○
Visible boundary between TZ and PZ representing compressed tissue
- ○
Frequently, calcified corpora amylacea (laminated bodies formed of secretions and degenerate cells) highlight plane between PZ and TZ
- ○
Zonal Distribution of Prostatic Disease
- •
Prostate adenocarcinomas
- ○
Up to 80% of prostatic cancers occur in PZ
- –
Most appear as hypoechoic lesions
- –
- ○
20% in TZ, 5% in CZ and are often indistinguishable from BPH
- ○
Signs of extraprostatic extension of prostatic carcinoma include asymmetry of neurovascular bundles and irregular bulge in prostatic contour
- ○
- •
BPH : Benign nodular hyperplasia in periurethral glands and TZ
- ○
Can cause bladder outlet obstruction from urethral compression &/or increased smooth muscle tone along bladder neck and urethra
- ○
Compresses PZ posteriorly
- ○
Periurethral gland hypertrophy creates what has been termed median lobe , which can be seen projecting into bladder on transabdominal scans
- ○
IMAGING ANATOMY
Ultrasound Technique
- •
Transabdominal ultrasound can assess size, but transrectal ultrasound (TRUS) is required for detailed assessment
- ○
Transducer
- –
3.5- to 6.0-MHz curved transducer for transabdominal ultrasound
- –
7- to 10-MHz rectal transducer (end firing or transverse panoramic)
- –
- ○
Patient position
- –
Transabdominal ultrasound: Supine, using urinary bladder as acoustic window (transvesical)
- –
TRUS: Left lateral decubitus with flexed hips and knees or in lithotomy position
- –
- ○
Transrectal biopsy of prostate
- –
Transrectal transducers have needle guidance system
- □
May be directed at lesion or in grid pattern covering prostate for random sampling
- □
- –
Complications include hematuria, hematochezia, hematospermia, and infection
- –
- ○
Color/power Doppler nonspecific; may see increased flow in hypertrophy, inflammation, and cancer
- –
Useful for directing biopsy
- –
- ○
- •
Normal PZ is typically uniformly more echogenic than inner gland
- ○
May be compressed in setting of BPH
- ○
- •
TZ may appear heterogeneous and nodular in setting of BPH
- •
Look for pseudocapsule (often with small calcifications) separating TZ from PZ
- •
Seminal vesicles have cystic appearance on TRUS, should be symmetric
- •
Prostate volume measurement
- ○
Perform in at least 2 orthogonal planes (axial and sagittal)
- ○
Prolate ellipse volume for 3 unequal axes: Width x height x length x 0.523
- ○
1 cc of prostate tissue weighs ~ 1 g; prostate weighs ~ 20 g in young men
- ○
Prostatic enlargement when gland is > 40 g
- ○
PROSTATE


VAS DEFERENS AND SEMINAL VESICLES

ZONAL ANATOMY OF THE PROSTATE
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


