Abstract
Gallstone ileus occurs when gallbladder stones erode and become lodged in the small bowel, thereby causing obstruction. These stones usually impact the terminal ileum because of its narrow lumen; however, they can also be found in less common locations, as observed in our case. The presence of pneumobilia can indicate gallstone ileus even without visible radiopaque stones because not all gallstones are detectable on computed tomography (CT). A 74-year-old woman presented to the emergency department with severe right upper quadrant pain that started 1 week previously and became more aggressive associated with fever, leukocytosis, and vomiting. The pain was colicky, intermittent, and aggravated by movement but did not radiate. Further imaging was requested to investigate the cause of the pain, which revealed evidence of proximal small bowel obstruction due to radiolucent gallstone ileus. Radiolucent gallstone ileus is a rare but serious condition requiring prompt surgical intervention. The presence of pneumobilia can indicate gallstone ileus even when the stones are not visible on CT. Large stones can cause blockages in the proximal small bowel. The ability of radiological imaging to detect gallstones varies according to their composition.
Introduction
Gallstone ileus is characterized by eroded gallbladder stones that are impacted in the small bowel, resulting in subsequent small bowel obstruction [ ]. The eroded stones typically impact the terminal ileum because of its relatively narrow lumen; however, these stones can be seen in atypical sites, as in our case [ ]. The presence of pneumobilia raises the suspicion of gallstone ileus even in the absence of radiopaque stones because not all gallstone types can be visualized on computed tomography (CT) [ ].
Case presentation
A 74-year-old woman presented to the emergency department with severe right upper quadrant pain that had begun 1 week earlier and progressively worsened. The pain was accompanied by fever, leukocytosis, and vomiting. She described it as colicky, intermittent, nonradiating, and aggravated by movement. On physical examination, the patient exhibited yellowish discoloration of the sclera (jaundice) and mild abdominal distention.
Due to the nonspecific clinical presentation, a contrast-enhanced CT scan was performed for further evaluation. The imaging revealed a large, dilated mid-jejunal loop with a maximum diameter of 3.2 cm ( Figs. 1 and 2 ) and a transition zone in the left anterior abdomen at the distal jejunal loops. Additionally, a partially distended gallbladder with internal air foci and a suspected fistulous connection to the first part of the duodenum was identified, along with pneumobilia. Notably, no hyperdense or calcified stones were observed.


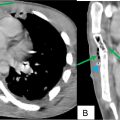
The CT scan also revealed an incidental finding of a mixed exophytic complex lesion in the right upper renal pole with an enhancing nodular component ( Fig. 3 ). This lesion was located near the right hepatic lobe, the right diaphragmatic crus, and the intercostal muscles between the 11th and 12th right ribs. Furthermore, a filling defect was noted within the right renal vein.

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Primary sternal osteomyelitis in an immunocompetent adolescent
Primary sternal osteomyelitis in an immunocompetent adolescent
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


