Abstract
Pulmonary sequestration is a congenital anomaly characterized by a mass of nonfunctioning lung parenchyma that receives a systemic arterial blood supply and is mainly located in the thorax. Intra-abdominal pulmonary sequestration, a rare subtype, is typically diagnosed within the first few months of life. We report the case of a term neonate with a history of recurrent left-sided pleural effusion requiring thoracentesis. A CT scan with venous contrast was performed, and an intrabdominal extralobar pulmonary sequestration was identified on the left, associated with a diaphragmatic hernia. The patient underwent embolization of the anomalous branch and reconstruction of the left diaphragm using bovine pericardium.
Introduction
Pulmonary sequestration (PS) is an uncommon congenital lung malformation, accounting for 0.15% to 6.4% of cases. It is characterized by a mass of nonfunctioning lung tissue that does not communicate with the normal tracheobronchial tree and is supplied by an anomalous systemic artery [ , ].
PS is classified into 2 main types—intralobar pulmonary sequestration (ILPS) and extralobar pulmonary sequestration (ELPS) —based on the presence of an independent visceral pleural covering [ , ] ( Fig. 1 ). PS may be asymptomatic and often diagnosed incidentally. Herein, we report a rare case of a 30-day-old newborn with intra-abdominal extralobar PS associated with left diaphragmatic agenesis.

Case report
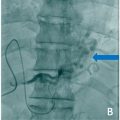
A term neonate without comorbidities had a history of recurrent left-sided pleural effusion requiring thoracentesis. A CT scan with venous contrast identified intra-abdominal extralobar PS and a left diaphragmatic hernia ( Fig. 2 ). Laboratory test results were within normal limits. The artery feeding the PS was embolized to reduce bleeding. In preparation for the embolization procedure, 20 mL of nonionic contrast medium (320 mgI/mL iodixanol) (4 mL/kg) and 20 mL of 0.9% saline solution (1:1 dilution) were administered. Access was gained through the right common femoral artery using a Slender 5 F introducer (Terumo) , followed by catheterization with a 4 F vertebral catheter (Terumo) and superselective microcatheterization with a Renegade STC microcatheter (Boston Scientific) and a Fathon 0.016” microguide (Boston Scientific). A diagnostic arteriogram revealed a hypervascular image of the PS without signs of a systemic venous shunt. Embolization was performed using 0.018” Interlock coils (2 × 4.1 cm, 2 × 2.3 cm and 2 × 5.8 cm) (Boston Scientific) , resulting in the devascularization of the accessory lung ( Fig. 3 ). The day after the embolization procedure, the patient underwent left thoracotomy with excision of the accessory lung and reconstruction of the diaphragm using bovine pericardium ( Fig. 4 ). The patient was discharged from the hospital after 4 days without complications. At 8 months of follow-up, the patient remained asymptomatic and showed appropriate development for his age.



Related posts:
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 Hepatic and extra-hepatic hydatid cysts: A case series of radiological and clinical insights
Hepatic and extra-hepatic hydatid cysts: A case series of radiological and clinical insights
 Percutaneous transhepatic embolization of gastro-esophageal varices for the treatment of variceal bleeding in portal vein thrombosis secondary to hepatocellular carcinoma: A case report
Percutaneous transhepatic embolization of gastro-esophageal varices for the treatment of variceal bleeding in portal vein thrombosis secondary to hepatocellular carcinoma: A case report
 Mid-term follow-up of a fractured flow diverter in the internal carotid artery
Mid-term follow-up of a fractured flow diverter in the internal carotid artery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


