Pulmonary vascular diseases, particularly when accompanied by pulmonary hypertension, are complex disorders often requiring multimodal imaging for diagnosis and monitoring. Echocardiography is the primary screening tool for pulmonary hypertension, while cardiac MR imaging (CMR) is used for more detailed characterization and risk stratification in right ventricular failure. Chest computed tomography (CT) is used to detect vascular anomalies and parenchymal lung diseases. While CT angiography is preferred for the detection of acute pulmonary embolus, dual-energy CT, single photon emission CT, and ventilation/perfusion scintigraphy are recommended for the detection of chronic thromboembolic disease. Application of these modalities will be reviewed here.
Key points
- •
Pulmonary vascular diseases, particularly when accompanied by pulmonary hypertension, are complex disorders that require multimodal imaging for diagnosis and subsequent monitoring.
- •
Although invasive right heart catheterization is required for definitive diagnosis and essential in pulmonary arterial hypertension, most patients with mild pulmonary hypertension never undergo catheterization. Rather, clinicians rely heavily on noninvasive cardiac and pulmonary vascular imaging studies to classify and risk-stratify patients.
- •
Mortality in pulmonary hypertension is largely determined by right ventricular function, making echocardiography and cardiac MR imaging critical for serial monitoring.
Introduction
Pulmonary hypertension (PH) is a complex and highly morbid disease characterized by either a primary pulmonary vasculopathy or, more commonly, secondary to pulmonary vascular remodeling due to cardiac, pulmonary, or other systemic conditions. PH is defined hemodynamically by a mean pulmonary artery (PA) pressure of greater than 20 mm Hg and is estimated to affect approximately 1% of the worldwide population. Patients with PH are grouped together based on clinical presentation, pathophysiology, and hemodynamics, with several recent updates to the hemodynamic classifications and thresholds ( Table 1 ). The most common causes are due to left heart disease followed by lung disease, while pulmonary arterial hypertension (PAH; Group 1) and chronic thromboembolic pulmonary hypertension (CTEPH; Group 4) are rare. Given the clinical overlap between these groups, multimodal diagnostic evaluation is required.
| PH Group | Common Clinical Etiologies | Hemodynamic Definition | Characteristic Imaging Findings |
|---|---|---|---|
| Group 1 | Idiopathic PAH Hereditable PAH Drug/toxin PAH CTD associated PAH Porto-pulmonary hypertension Congenital heart disease PVOD | mPAP >20 mm Hg PAWP ≤15 mm Hg PVR >2 WU |
|
| Group 2 | HFpEF HFrEF Valvular heart disease | mPAP >20 mm Hg PAWP >15 mm Hg |
|
| Group 3 | Lung diseases, that is, COPD, ILD Developmental lung diseases Hypoxia Hypoventilation syndromes | mPAP >20 mm Hg PAWP ≤15 mm Hg |
|
| Group 4 | CTEPH Other pulmonary artery obstructions | mPAP >20 mm Hg PAWP ≤15 mm Hg PVR >2 WU |
|
| Group 5 | Unclear or multifactorial mechanisms, clinically includes myeloproliferative disorders, metabolic disorders, sarcoidosis, Langerhans cell histiocytosis, neurofibromatosis, fibrosing mediastinitis, ESRD | Varies by etiology | Varies by etiology |
Although invasive right heart catheterization is required for definitive diagnosis and essential in PAH, most patients with mild PH never undergo catheterization. Rather, clinicians rely heavily on noninvasive imaging to classify and risk-stratify patients. Echocardiography is the most widely employed imaging modality for screening for PH and provides initial clues to etiology and severity. Integration of additional imaging modalities is necessary in the comprehensive evaluation of PH. , Cardiac MR imaging (CMR) provides additional diagnostic assessment and risk stratification of right ventricular (RV) failure. Computed tomography (CT) and ventilation/perfusion (V/Q) scintigraphy allow for assessment of the pulmonary and mediastinal structures as well as pulmonary blood flow. Pulmonary angiography can supplement these modalities and is primarily used in the work-up of CTEPH, as well as in the evaluation of pulmonary arteriovenous malformations, pulmonary stenosis, and intrapulmonary shunts. Understanding the advantages and disadvantages these available tools is critical for the diagnosis and follow-up of patients with PH. Insights gained by these imaging studies enhance our understanding of the physiology of pulmonary vascular disease. This review focuses on the clinical use of key imaging modalities in pulmonary vascular diseases, particularly PH, for proper classification, risk assessment, and treatment.
Echocardiography
Echocardiography is the primary imaging modality for both the initial diagnosis and serial follow-up of PH. It is a widely available, reliable, and cost-effective tool to evaluate cardiac structure and function. Guidelines recommend echocardiography to screen for PH, with the probability of PH based on tricuspid regurgitant velocity (TRV) and other echocardiographic findings. RV systolic pressure measured using Doppler of the TRV is used to estimate PA systolic pressure. A TRV greater than 3.4 m/s suggests a high probability of PH, while a TRV less than 2.8 m/s suggests a low probability. This method relies on an adequate acoustic window, appropriate Doppler beam alignment, as well as sufficient tricuspid regurgitation for an adequate Doppler envelope to estimate TRV and thus is not achievable in all patients. The initial screening echocardiogram also includes a comprehensive evaluation of cardiac structures (valves, atrial and ventricular septum, etc.) and function, which can provide clues as to the origin of PH. Evaluation of the left ventricle (LV) for left heart disease is essential for diagnosing Group 2 PH. Based on this initial screening, further imaging and diagnostic cardiac catheterization are pursued.
Several features beyond TRV suggest PH, many of which are also visible on other imaging modalities more commonly interpreted by radiologists. Measurement of the RV volume in systole and diastole in the 4 chamber view can be used to calculate a fractional area change (FAC) as a quantitative measure of RV systolic function, where a FAC less than 35% indicates RV systolic dysfunction. Right atrial (RA) area should be calculated from the 4 chamber view, as an RA area greater than 26 cm 2 predicts a poor outcome. The basal dimensions of the RV and LV in the 4 chamber or parasternal short axis views should be compared, with an elevated RV:LV ratio strongly associated with worse outcomes. In adults, an RV:LV dimension greater than 1 is considered abnormal, while in pediatrics, an increasing RV:LV ratio predicts progressively worse outcomes. , Flattening of the interventricular septum, often termed a “D-shaped septum,” is a strong indicator of RV pressure overload and suggests PH. Any of these findings require additional diagnostic evaluation.
For patients with PH, risk stratification models such as the (Registry to Evaluate Early and Long-Term PAH Disease Management [REVEAL]) 2.0 score and the European Respiratory Society risk criteria include multiple echocardiographic parameters of RV size and function. , RA area, tricuspid annular plane systolic excursion, and presence of a pericardial effusion continue to show the best prognostic value and are used for risk assessment. Presence and size of a pericardial effusion should always be documented as this remains one of the best indicators of RV failure and may require aggressive acute management. Serial echocardiograms are used to guide therapy with the goal being to target low risk status for the best long-term prognosis. ,
Cardiac MR imaging
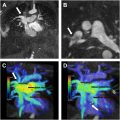
Cardiac MR imaging (CMR) is considered the reference-standard for imaging the RV. While CMR is not used routinely for the initial diagnosis of PH in many centers, its superior resolution and characterization of cardiac structure and function allow for precise and repeatable evaluations of RV function, volumes, and mass. Clinically, CMR is frequently used for evaluation of cardiac diseases associated with PH (eg, congenital heart disease and infiltrative cardiomyopathies) and serially for risk stratification and response to medical therapy. Steady-state free-precession sequences provide accurate analysis of biventricular structure and function, classically showing RV dilation and hypertrophy. Septal bowing and left atrial (LA) or LV compression suggest RV pressure overload states commonly seen in PAH. Late gadolinium enhancement (LGE) frequently identifies increased collagen deposition at the RV insertion points, with greater mass of LGE associated with worse hemodynamic profiles in PAH. LA or LV dilation, reduced LV ejection fraction, and impaired LV diastolic function suggest Group 2 PH. Two dimensional phase-contrast imaging is used to assess PA hemodynamics, including mean PA velocity, pulse wave velocity, and relative area change, all markers of PA stiffness. Proximal PA stiffness, assessed by PA relative area change from systole to diastole, also predicts increased mortality risk in PAH. Additional novel metrics capture PA–RV mechanical coupling, a measure of RV contractile function relative to afterload, and are also associated with increased mortality risk. The most utilized index in CMR is a volumetric method defined as RV stroke volume/RV end-systolic volume, though measures of LV eccentricity and RV strain are increasingly utilized to assess ventricular–vascular coupling.
RV failure is a key determinant of prognosis and mortality in PH, and CMR is included many risk assessment models. CMR is also used to define treatment-associated functional recovery in patients with PAH and is more sensitive than classically followed PAH outcome parameters such as 6 min walk distance and (N-terminal pro b-type natriuretic peptide [NT-proBNP]). , A meta-analysis of 22 studies by Alabed and colleagues demonstrated that every 1% decrease in RV ejection fraction was associated with a 4.9% increase in risk for clinical worsening (defined as hospitalization, disease progression, or mortality) and a 2.1% increased risk of death. Further, a 1 mL/m 2 increase in RV end-systolic volume index or RV end-diastolic volume index increased risk of clinical worsening by 1.3% and 1%, respectively. With respect to treatment response, a 5% absolute increase in RV ejection fraction and a 17 mL decrease in RV end-diastolic or end-systolic volumes were identified as the minimally important differences associated with improvement in overall patient symptoms, daily functioning, and survival. However, a 5% decrease in RV ejection fraction or 10 mL increase in RV volumes was associated with clinical worsening. A recent study also suggested 1 year follow-up CMR-based risk assessment is at least non-inferior to invasive catheterization-based risk assessment, supporting its growing use.
Other novel applications of CMR in PH include use of PET/MR imaging to assess myocardial metabolism, simultaneous measurement of invasive hemodynamics, and application of in-scanner exercise programs. Novel multi-parametric CMR models are now being used to estimate mean PA pressure with reasonable diagnostic accuracy, though these methods have not yet reached clinical practice. Furthermore, the ability to distinguish high versus low pulmonary capillary wedge pressure (and thus PAH from Group 2 PH or mixed PH) will be critical if CMR is to supplant right heart catheterization.
Chest radiography
While chest radiography has a limited role in elucidating the etiology of pulmonary vascular disease, it remains an important and cost-effective tool to suggest need for additional evaluation. Frequently abnormal at the time of initial diagnosis, chest radiographs may show an enlarged cardiac silhouette, PA dilation, or pruning of peripheral vessels. , The identification of Kerley B lines or pleural effusion may prompt consideration of pulmonary venous hypertension due to left heart disease (Group 2 PH), while significant reticulation or emphysema may suggest PH due to lung disease (Group 3 PH). The utility of chest radiography should not be underestimated, particularly in resource-poor settings where more advanced imaging modalities may be less accessible.
Computed tomography
CT has secured a crucial position in the evaluation of pulmonary vascular disease. It offers a swift assessment of cardiac, mediastinal, vascular, and pulmonary structures, using high-spatial-resolution isovolumetric imaging. Three CT variations are commonly used in contemporary practice: unenhanced CT imaging, CT angiography (CTA), and high-resolution CT imaging (HRCT). In this section, we will also review dual-energy CT (DECT) and single photon emission computed tomography (SPECT) as imaging techniques with evolving utility.
Unenhanced Computed Tomography and High-resolution Computed Tomography
Distinct abnormalities may be indicative of specific disorders and have notably unique imaging findings on unenhanced and HRCT images. These include signs of emphysema, interstitial lung disease, pulmonary Langerhans cell histiocytosis, or pulmonary sarcoidosis, all of which can lead to PH. An anatomic assessment using HRCT can aid in the severity of underlying lung disease, though there is no significant correlation between mean PA pressures and the extent of parenchymal lung disease or fibrosis seen on CT imaging. There are several features and characteristic findings on CT that must be highlighted given their presence in Group 1 PAH, including the development of centrilobular nodules, peripheral neovascularization, and lobular areas of ground-glass attenuation.
Computed Tomography Angiography
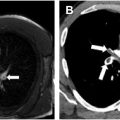
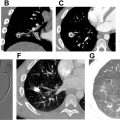
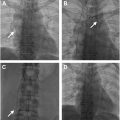
CT pulmonary angiography (CTPA) is a specialized application of CT scans in which contrast administration is precisely timed to enhance opacification of the pulmonary arteries. Often completed for evaluation of dyspnea or hemoptysis, features suggestive of PH include the following: PA dilation, tortuosity of the PAs, rapid tapering of the PAs, mosaic attenuation of the lung parenchyma, contiguous reflux of contrast into the inferior vena cava, RV dilation, RV hypertrophy, flattening of the intraventricular septum, and dilation of the bronchial arteries ( Fig. 1 ). , ,

Related posts:
 Pathology of Pulmonary Vascular Disease with Radiologic Correlation
Pathology of Pulmonary Vascular Disease with Radiologic Correlation
 Imaging of Acute Pulmonary Embolism
Imaging of Acute Pulmonary Embolism
 Imaging of Pulmonary Vasculitis
Imaging of Pulmonary Vasculitis
 Congenital Pulmonary Vascular Anomalies and Disease
Congenital Pulmonary Vascular Anomalies and Disease
 Role of Cardiovascular MR Imaging and MR Angiography in Patients with Pulmonary Vascular Disease
Role of Cardiovascular MR Imaging and MR Angiography in Patients with Pulmonary Vascular Disease
 Pulmonary Vascular Interventions
Pulmonary Vascular Interventions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


