MR imaging is currently the main imaging modality used for the diagnosis and post therapeutic assessment of glioblastomas. Recently, several innovative PET radioactive tracers have been investigated for the evaluation of glioblastomas (GBM). These radiotracers target several biochemical and pathophysiological processes seen in tumors. These include glucose metabolism, DNA synthesis and cell proliferation, amino acid transport, cell membrane biosynthesis, specific membrane antigens such as prostatic specific membrane antigens, fibroblast activation protein inhibitor, translocator protein and hypoxia sensing agents, and antibodies targeting specific cell receptor antigen. This review aims to discuss the clinical value of these PET radiopharmaceuticals in the evaluation and treatment of GBMs.
Key points
- •
The role of F18-FDG PET in the evaluation of glioblastoma and high-grade gliomas and monitoring treatment response.
- •
Amino acid PET tracers (C11-methionine, F18-FDOPA, F18-fluciclovine) for the evaluation of brain tumors and the differentiation of tumor recurrence from treatment related changes.
- •
PSMA-targeted PET imaging radiotracers in assessing glioblastoma and high-grade gliomas, the potential role in the radiation therapy planning, and the complementary role of theranostics.
- •
Fibroblast activation protein (FAP) inhibitor (FAPI) based PET imaging and the potential of FAPI-based theranostics in the management of GBM.
- •
PET radiotracer for the assessment of hypoxia and PET imaging of the immune system.
Introduction
Glioblastoma multiforme (GBM) is the most aggressive adult central nervous system (CNS) neoplasm with poor prognosis and a mean survival time of 15 months. Pathologically, the isocitrate dehydrogenase (IDH) wild-type GBM carries a worse prognosis and shorter survival period than the IDH mutant type GBM. Current treatment of GBM consists of surgical resection followed by radiation and chemotherapy. , However, GBM has a high recurrence rate due to its resistance to radiotherapy and chemotherapy.
MR imaging is the predominant clinical imaging modality for the diagnosis and post therapeutic assessment of glioblastomas. MR imaging utilizes multiple sequences, including the T2-weighted sequence, fluid attenuated inversion recovery (FLAIR), pre-gadolinium and post-gadolinium T1-weighted sequences, diffusion weighted imaging, diffusion tensor imaging, perfusion imaging, MR spectroscopy, and functional MR imaging. However, the interpretation of MR imaging, specifically for the accurate detection of glioma recurrence, is often influenced by treatment-related effects such as concomitant radiation necrosis, pseudo progression, or pseudo response, which restricts clinicians from making appropriate management decisions of these patients.
In recent years, there has been a substantial increase in the number of publications regarding PET tracers for the evaluation of GBMs. These PET radiotracers target different biochemical and pathophysiological processes, involving glucose metabolism, DNA synthesis and cell proliferation, amino acid transport, cell membrane biosynthesis, radiolabeled targeting of specific membrane antigens such as prostatic-specific membrane antigen (PSMA), fibroblast activation protein inhibitor (FAPI), and hypoxia-sensing agents ( Table 1 ).
| Radiotracer | Mechanism of Radiotracer |
|---|---|
| F18-2-fluoro-2-deoxy- d -glucose (F18-FDG) | Glucose metabolism |
| 3′-deoxy-3′- 18 F-fluorothymidine (F18-FLT) | DNA synthesis and cell proliferation |
| C11-methionine (C11-MET) | Amino acid metabolism |
| 3,4-dihydroxy-6-F18-fluoro- l -phenylalanine (F18-FDOPA) | Amino acid metabolism |
| O-(2-F18-fluoroethyl)- l -tyrosine (F18-FET) | Amino acid metabolism |
| F18-flurocyclobutane- 1 -carboxylic acid F18-FACBC, F18-fluciclovine | Amino acid metabolism |
| Ga68-PSMA-11 | Targeting transmembrane PSMA protein |
| Ga68-FAPI PET radiotracer | Targeting the fibroblast activation protein |
| F18-fluoromisonidazole (F18-FMISO) | Hypoxia-sensing agent |
| C11-choline | Cell membrane synthesis |
Whole body 3 dimensional PET imaging with these PET tracers is complementary to conventional MR imaging and enables the noninvasive evaluation of tumor avidity, recurrence, distal metastasis, as well as the evaluation of the microenvironment such as the presence of anoxia that may preclude an adequate response to current therapy.
F18-2-fluoro-2-deoxy- d -glucose PET imaging
F18-2-fluoro-2-deoxy- d -glucose (F18-FDG) is a glucose analog and transported through the glucose transporter into the cytosol where it is phosphorylated by hexokinase and trapped inside the cell as fludeoxyglucose (FDG)-6 phosphate. High-grade tumors demonstrate increased rates of glycolysis and cellular proliferation, and F18 FDG is the most widely utilized radiotracer in high-grade tumors such as GBMs for diagnosis, staging, and monitoring response to therapy. As early as 1982, FDG-PET was utilized in the evaluation of human cerebral gliomas. Since then, newer PET radiotracers have been developed for the detection of gliomas as well as to evaluate treatment response.
In addition to qualitative imaging, quantitative analysis in patients with glioblastoma can be performed using the maximum standardized uptake value (SUVmax), and the ratio of lesion SUVmax to the mean standardized uptake value (SUVmean) of contralateral white matter (SUVmax/WM). Studies have shown a negative correlation between SUVmax alone and SUVmax/WM with patient survival. Whole-body F18-FDG PET/computed tomography (CT) is able to detect extracranial metastasis in patients with primary GBM.
Quantitative evaluation of F18-FDG PET with the tumor-to-contralateral normal brain tissue ratio 2.4 or greater appears specific for primary CNS lymphoma, providing 83.8% sensitivity and 95.2% specificity, potentially helpful for differentiating primary CNS lymphoma from GBM.
Radiomics and artificial intelligence are recent emerging techniques that extract high-throughput imaging features from standard PET imaging and provides additional information by computational processing such as texture analysis, , assesses the tumor heterogeneity that is related to biologic tumor features, and provides additional predictive and prognostic information. F18-FDG PET-based radiomics approach has been successfully proven useful to distinguish GBM from primary CNS lymphoma.
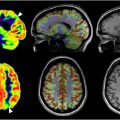
F18-FDG PET is also useful to monitor treatment response for GBM. The other advantage of F18-FDG PET is the ability to differentiate GBM recurrence from treatment related changes, such as pseudo progression and radiation necrosis. In the evaluation of IDH-wild-type glioblastoma, delayed F18-FDG PET imaging at 5 and 8 hours post-FDG injection demonstrated significant higher tumor to background ratio compared to conventional imaging acquired at 1 hour post-F18-FDG injection ( Fig. 1 ). Future research based on delayed F18-FDG PET may have the potential to improve the discrimination between true progression and pseudo progression.

Bevacizumab, a vascular endothelial growth factor receptor antagonist, has been utilized for the treatment of recurrent GBM. In a retrospective study, bevacizumab was administered to patients suspected of having recurrent GBM and disease progression. The patients were followed up with brain F18-FDG PET within 4 weeks of receiving bevacizumab. The median overall survival (OS) was 9.0 months in patients with non-FDG avid versus 4.5 months in patients with FDG avid. SUVmax, peak standardized uptake value (SUVpeak), and tumor-to-normal contralateral white matter ratios were significantly associated with OS ( P <.001, TLG: P =.009). Additionally, quantitative PET/MR imaging parameters in combination with dynamic susceptibility contrast perfusion MR imaging have been reported to facilitate distinguishing radiation necrosis from tumor recurrence in treated GBMs.
3′-Deoxy-3′-F18-fluorothymidine
Thymidine is a nucleoside in DNA synthesis. Human cancer cells demonstrate upregulation of nucleotide metabolism, and could be evaluated via radioisotope labeled thymidine. As early as 1992, C11-thymidine was shown taken up in patients head and neck tumors. However, this tracer is limited by the short half-life of C11. Later, 3′-deoxy-3′-F18-fluorothymidine (F18-FLT) was developed for PET imaging. Fluorothymidine (FLT) is an analog of thymidine; F18-FLT enters proliferating human tumor cells both via a nucleoside transporter and partly via passive diffusion. , F18-FLT cellular retention is mediated by phosphorylation by the enzyme thymidine kinase 1 and then F18-FLT is trapped intracellularly. FLT is only slightly able to cross the intact blood–brain barrier and demonstrates very low background uptake in the normal brain tissue. Therefore, F18-FLT PET is superior to F-18 FDG PET that has high rate of physiologic glucose metabolism in the normal brain tissue and high background uptake.
High-grade gliomas and other brain tumors associated with significant blood–brain barrier breakdown demonstrate significant F18-FLT uptake. FLT uptake has been shown to correlate with cancer cell proliferation in high grade gliomas. In a study of patients with newly diagnosed gliomas, a significant correlation was found between F18-FLT uptake tumor to contralateral normal brain tissue (T/N) ratio and Ki-67 index on Ki-67 immunohistochemistry. A prospective study showed that grade IV gliomas demonstrated the highest F18-FLT uptake, the maximum value of F18-FLT uptake (FLTmax) was the most relevant parameter for the discrimination of grade II from grade IV gliomas and the differentiation of grade III from grade IV gliomas, and FLTmax had the best correlation with the preoperative grade of gliomas ( Fig. 2 ).

F18-FLT PET imaging plays an important role in the evaluation of treatment response of GBM and recurrent malignant gliomas. A pilot human study employed F18-FLT PET to assess treatment response of recurrent malignant gliomas to bevacizumab in combination with irinotecan and showed that metabolic responders demonstrated longer survival than nonresponders. Another clinical study evaluated therapy effect of bevacizumab on patients with recurrent malignant glioma and showed that F18-FLT PET seemed superior to MR imaging in the prediction for early treatment response. A clinical study further showed that lower baseline F18-FLT PET uptake was associated with improved survival in patients with GBM after chemoradiotherapy.
Amino acid PET imaging
Radiolabeled amino acids are under active clinical investigation for the evaluation of CNS tumors. The most reported amino acid tracers are C11-methionine (C11-MET), 3,4-dihydroxy-6-18F-fluoro- l -phenylalanine (F18-FDOPA), O-(2-F18-fluoroethyl) – l -tyrosine(F18-FET), and F18-flurocyclobutane-1-carboxylic acid (F18-FACBC, F18-fluciclovine). These tracers are taken into the cells mainly through the neutral amino acid transporters of the L-type (LAT) in gliomas and brain metastases. These tracers are helpful for differentiation of tumor recurrence from treatment-related changes such as radiation necrosis or pseudo progression, as well as guiding treatment planning.
C 11-Methionine
In comparison to glucose, most cancers are more avid or dependent on methionine, and glioblastoma tumors demonstrate specific affinity for methionine. C11-MET PET has been shown to be more sensitive and accurate than F18-FDG PET for the detection of GBM and other cancers in the brain.
Patients with GBM who showed high accumulation index of C11-MET had shorter OS. Patients with GBM who underwent surgical resection of the PET positive tissue on C11-MET PET have shown significantly prolonged survival. It should be noted that in patients with GBM, the preoperative C11-MET PET volume generally was greater than the enhancing lesion on the preoperative MR imaging; therefore, it should be taken into consideration during the surgical planning in order to achieve a supra total resection. In addition, a study evaluating glioma IDH mutation status showed that the positive C11-MET PET imaging in combination with the MR imaging T2-FLAIR mismatch sign demonstrated improved diagnostic accuracy to determine glioma molecular subtype.
C11-MET PET has also been shown to be helpful in the discrimination of tumor progression from treatment-related changes. A clinical study employed receiver-operating characteristic analysis and area under the curve calculations. This study revealed that using C11-MET PET, the maximum tumor-to-background ratios (TBRmax) had the best performance in differentiating tumor progression from treatment-related changes with a cut-off of 2.13 in IDH-wild-type glioblastoma.
C11-MET PET could detect both IDH-wild-type GBM and primary CNS lymphoma but cannot discriminate between these 2 major types of brain tumors.
Dihydroxy-6-18F-Fluoro- l -Phenylalanine
Dihydroxy-6-F18-fluoro- l -phenylalanine (F18-DOPA) is another recently investigated amino acid analog radiotracer in the detection of GBM. l -Amino acid transporter 1 (LAT1) and the mitochondrial translocator protein are overexpressed in GBM. It has been thought that F18-DOPA uptake is related to LAT1 expression. IDH-mutant gliomas had higher LAT1 expression than IDH-wild-type gliomas. Among the World Health Organization (WHO) grade 4 gliomas, IDH-mutant astrocytoma demonstrated higher F18-DOPA uptake with higher TBRmax than IDH-wild-type GBM ( Fig. 3 ). The ratio of maximum F18-DOPA SUV in tumor to normal tissue (T/N SUVmax) was reported significantly greater in glioblastoma (WHO IV) than lower grade gliomas (WHO I-III).

A recent study utilizing radiomic modeling of F18-DOPA PET imaging achieved 80% ± 10% accuracy for 95% confidence level in the prediction of O6-methylguanine-DNA methyltransferase (MGMT) status for patients with GBM. Compared to MR imaging, F18-DOPA PET detected substantially larger tumor volumes for patients with GBM.
A phase 2 clinical trial study showed that F18-DOPA PET-guided dose-escalated radiation therapy was safe, significantly prolonged the progression-free survival (PFS) in patients with MGMT unmethylated GBM, and prolonged the OS in patients with MGMT methylation.
O-(2-[18F]-Fluoroethyl)- l -Tyrosine
F18-fluroethyltyrosine (F18-FET) is another amino acid analog radiolabeled with fluorine F18 and is transported into tumor cells via system-L amino acid transporter. F-18 FET has favorable features, including high metabolic stability in vivo, high tumor to background contrast, and tissue-specific uptake kinetics.
Dynamic F18-FET PET studies were performed in patients with glioma to evaluate the course of F18-FET uptake overtime. The time-activity curves of F18-FET uptake showed that high-grade gliomas often exhibited an early peak around 10 to 20 minutes after radiotracer injection followed by a decrease of FET uptake, in contrast to low-grade gliomas that usually showed delayed and steadily increased FET uptake. , These different patterns of time-activity curves of FET uptake provide additional information on the differential diagnosis and tumor grading.
F18-FET PET/CT appears superior to the contrast MR imaging for the initial diagnosis of GBM and other primary brain tumors with higher sensitivity (100% vs 52.9%) and higher negative predictive value (100% vs 38.4%).
The recent application of artificial intelligence and deep learning-based F18-FET PET segmentation is able to perform reliable, robust, and fully automated evaluation of metabolic tumor volume (MTV) in patients with brain tumor. A decrease of MTV was a significant predictor of disease-free survival and OS in patients with glioma.
A retrospective analysis of F18-FET PET imaging was performed on patients who had gadolinium enhancement on MR imaging and were suspicious of recurrent glioblastoma and considered for salvage surgery. Forty-two of the 51 patients who underwent F18-FET PET received a second surgery. Final neuropathology confirmed tumor recurrence in each case. This study suggested that F18 FET-PET scan can be a potential selection tool for candidates with glioblastoma recurrence for salvage surgery.
A small case series evaluated the effect of immunotherapy with dendritic cell vaccination in patients with GBM. In some patients, MR imaging findings indicated tumor progression, and in contrast, the F18-FET PET imaging indicated treatment-related changes. This suggests that F18-FET PET imaging is able to monitor the response to GBM immunotherapy.
F18-Flurocyclobutane-1-Carboxylic Acid
F18-FACBC, F18-fluciclovine, also known as Axumin, is a PET radiotracer utilized to evaluate men suspicious of recurrent prostate cancer in patients with prostate specific antigen (PSA) biomedical recurrence. , It is rare to observe intracranial uptake of F18-fluciclovine, and the differential diagnosis includes prostate cancer brain metastasis versus primary brain tumor. It has been demonstrated that fluciclovine is transported into human astrocytes and glioma cells utilizing the amino acid transporter system LAT1 and alanine serine cysteine transporter 2.
Several types of brain tumors have been reported to accumulate fluciclovine, the most frequently reported cases are glioma, although other types of tumor have also been reported positive on F18-Fluciclovine PET such as meningioma, anaplastic oligodendroglioma, and pituitary adenoma. The first human case of residual GBM performed as early as 1999 utilizing F18-Fluciclovine PET demonstrated a high tumor-to-normal-tissue ratio of F18-Fluciclovine uptake. A phase IIa clinical study reported positive F18-Fluciclovine uptake in 5 patients with malignant glioma, and F18-Fluciclovine PET/CT showed more extensive regions of tumor than the post-contrast T1-weighted MR imaging. F18-Fluciclovine PET was shown to facilitate the differential diagnosis between high-grade glioma and low-grade glioma. Both SUVmax and the ratio of tumor to background F18-Fluciclovine uptake had a high statistical correlation with the tumor proliferative index Ki-67 ( Fig. 4 ). When compared to C11-MET PET, the F18-Fluciclovine PET showed higher lesion to contralateral normal brain tissue ratios.

Glioblastoma patients with tumor progression had a significantly higher SUVmax of F18-fluciclovine uptake (6.64 + 1.88) than patients with pseudo progression (4.11 ± 1.52, P =.009), suggesting that F18-fluciclovine uptake has clinical value in differentiating GBM tumor progression from pseudo progression.
A study in patients undergoing chemoradiotherapy for GBM has shown that the tumor volumes of F18-fluciclovine activity detected outside of the dynamic contrast-enhanced MR imaging and post-contrast T1-weighted MR imaging were associated with poorer prognosis and shorter OS.
Prostate-specific membrane antigen PET imaging
PSMA is a cell membrane protein that is highly expressed in prostate cancer cells. Apart from its expression in prostate tissue, PSMA has been proven to be expressed in other types of cancers, such as gliomas, renal cell carcinoma, and breast cancer. As for the gliomas, PSMA immunostaining of the formalin-fixed, paraffin-embedded tissue blocks of high-grade gliomas revealed that PSMA is expressed in the neovasculature of high-grade gliomas, especially in the endothelial cells of tumor microvessels and in parenchymal tumor cells.
The Food and Drug Administration (FDA) has approved 4 PSMA-targeted PET imaging radiotracers, Ga68-PSMA-11, Ga68 gozetotide (Locametz), F18-piflufolastat (Pylarify), and F18-flotufolastat (Posluma) for men with prostate cancer. The expression of PSMA in high-grade gliomas provides a rationale to investigate PSMA-targeted PET imaging radiotracer for the diagnosis of brain tumors specifically high-grade gliomas.
Recently, there have been reports about the detection of GBM utilizing Ga68-PSMA PET/CT ( Fig. 5 ). , As early as 2017, studies compared Ga68-PSMA-11 PET/CT to F18-FDG PET/CT scan in the evaluation of treated patients with GBM suspicious of recurrence. A good correlation was observed between Ga68-PSMA-11 PET/CT and F18-FDG PET/CT. Further, Ga68-PSMA-11 PET/CT demonstrated significant high target to background ratio and better visualization of the recurrent lesion, superior to F18-FDG PET/CT.

A prospective study of 15 patients utilizing Ga68-PSMA-11 showed increased uptake in high-grade gliomas with good tumor-to-background ratio, SUVmax values were significantly elevated in higher-grade tumors, and SUVmax values were higher in those tumors with high Ki-67 indices. Additionally, the IDH mutation wild-type glioma showed higher SUV max values.
Another prospective clinical study compared Ga68 PSMA-617 and F18-FET PET in 10 patients with recurrent GBM. The tumor volume detected with Ga68 PSMA-617 PET was larger than F18-FET PET. The tumor volume detected with Ga68 PSMA-617 PET was also larger than that assessed via MR imaging contrast enhancement. Ga68 PSMA-617 PET had significantly higher tumor-to-brain ratio than F18-FET PET ( P =.002). The tissue accumulating Ga68 PSMA-617 outside of the F18-FET avid tissue is likely related to the neo-angiogenesis process.
A meta-analysis and systematic review was performed about studies on the diagnostic accuracy of PET/CT or PET/MR imaging employing PSMA-targeting radiopharmaceuticals in high-grade gliomas; 157 patients were included in the meta-analysis. This study reported a sensitivity of 98.2% and specificity of 91.2%, suggesting high diagnostic accuracy of high-grade glioma utilizing PSMA-targeting PET/CT or PET/MR imaging.
A study compared Ga68-PSMA-11 to F18-DOPA PET/CT for the detection of early recurrence in patients with GBM. Tumor recurrence cases showed increased Ga68-PSMA-11 uptake and were better visualized than the F18-DOPA PET/CT. Postradiation-related changes displayed relative lower uptake of Ga68 PSMA-11 than F18-DOPA, indicating the potential utility of Ga68-PSMA-11 PET/CT for the differentiation of postradiation inflammation from tumor recurrence. Similarly, the region of radiation necrosis on MR imaging did not show Ga68-PSMA-11 radiotracer accumulation, which is helpful in the differentiation of radiation necrosis from recurrent glioma.
Ga68-PSMA PET may have a potential role in the radiation therapy planning. A study retrospectively utilized the contour of Ga68-PSMA uptake area as the biologic tumor volume (BTV), and compared to the gross tumor volume (GTV) contoured from the contrast-enhanced area in T1-weighted MR imaging, and found that the BTV was larger than GTV, suggesting that Ga68-PSMA PET may help defining the non-enhancing MR imaging tumor compartment.
2-(3-{(1carboxy-5-[(6-[F18]-fluoro-pyridine-3-carbonyl)-amino]-pentyl)}-ureido)-pentanedioic acid, abbreviated as F18-DCFPyL, is a molecule targeting PSMA. It was reported to bind PSMA in the neovasculature of GBM and tumor cells of anaplastic astrocytoma. GBM was positively detected in the F18-DCFPyL PET.
Fibroblast activation protein inhibitor-based PET imaging
Fibroblast activation protein α (FAP) is a type-II transmembrane serine protease that is highly expressed on cancer-associated fibroblasts (CAFs) in the majority of epithelial cancers. FAP is increasingly expressed in GBM both by tumor cells and stromal cells CAFs and contributes to diffuse glioma invasion. Specifically, FAP is expressed in the mesenchymal subtype of GBM and promotes GBM angiogenesis.
PET imaging targeting the FAP inhibitor is a strategy that targets the CAFs. Among the many developed FAPI-based radiotracers, gallium 68-labeled FAPIs (Ga68-FAPIs) PET radiotracer demonstrates specific binding to FAP. There is rapid tracer accumulation in target lesions, and low background signal, providing the most favorable imaging features, and enabling the detection of a variety of primary tumors and metastatic lesions. FAPI PET/CT has been reported able to detect GBM, sarcoma, breast cancer, lung cancer, and various other types of cancers.
GBM has been reported to be positive on Ga 68-FAPI PET imaging by several groups. , As early as 2019, a group reported increased Ga68-FAPI-02/04 uptake in IDH-wild-type glioblastomas and grade III/IV IDH-mutant gliomas at 30 minute post-intravenous administration of radiotracer. Another tracer is Ga68-FAPI-46, which has a favorable dosimetry profile, and demonstrates high lesion uptake with high tumor-to-background ratios, rapid body clearance, and low accumulation in normal tissues.
In addition, researchers developed another tracer [68 Ga]Ga-Alb-FAPtp-01, which also showed prominent tumor uptake overtime and improved pharmacokinetics. Utilizing a xenograft mouse model of GBM established by inoculation of U87MG tumor cells—a human glioblastoma cell line, [68 Ga]Ga-Alb-FAPtp-01 was able to noninvasively detect FAP activation in vivo. The tumor contrast ratio of tumor/muscle increased continuously from 1 hour up to 3 hours post-radiotracer injection.
Similar to Ga68-FAPI PET imaging, there is also a report about GBM in F18-FAPI PET/CT. A recent clinical study compared F18-FAPI PET/CT to MR imaging in assessing patients with GBM. This study showed that F18-FAPI PET/CT had a sensitivity of 69.6% and positive predictive value of 100%, and the SUVmax of the GBM was 7.08 ± 3.55 and tumor-to-background ratio was 19.95 ± 13.22.
FAPI PET/CT has more advantages than FDG PET/CT in detecting primary and metastatic lesions. Compared to F18-FDG PET/CT, diet or fasting is not necessary for the preparation for FAPI PET/CT examination.
PET radiotracer for the assessment of hypoxia
The current standard treatment of GBM is surgery followed by chemotherapy and radiation. However, GBM frequently demonstrates resistance to radiation therapy and temozolomide (TMZ) and tumor recurrence may occur. ,
Hypoxic tumor microenvironment has been associated with the resistance of GBM to standard therapy. The intratumoral hypoxic gradient has been correlated with the tumor cell phenotype, drives stem cells distribution, and has been correlated with chemotherapy resistance. GBMs show increased hexokinase 2 expression and correlate with worse OS of patients with GBM. In vitro study evaluating different oxygen levels to TMZ-resistant GBM cells showed that hyperoxia increased TMZ toxicity in GBM cells. In addition, hypoxic tumor environment stimulates GBM cellular plasticity toward a stem-like phenotype that is associated with treatment resistance. ,
The assessment of hypoxia with advanced PET tracer provides significant clinical value in the detection of hypoxia and treatment-resistant GBM. To date, F18-fluoromisonidazole (FMISO) is the most extensively investigated radiotracer for hypoxia imaging. , As early as 2008, a study utilizing F18-FMISO PET in patients with GBM showed shorter time to progression and shorter survival times in patients whose tumors contained higher hypoxic volumes.
Another research utilized F18-FMISO PET and MR imaging including relative cerebral blood volume (rCBV) maps in patients with glioma before surgery. It found a correlation between the degree of hypoxia and rCBV in MR imaging, as well as the correlation between the degree of hypoxia and the expression of molecules related to angiogenesis.
A study evaluated tumor hypoxia with F18-FMISO PET in patients with recurrent GBM refractory to bevacizumab. This study showed that hypoxic volume detected with F18-FMISO PET was negatively correlated with the PFS and OS, and the reduction in hypoxic volume was correlated with longer PFS and OS.
A case series report involved patients with newly diagnosed IDH-wild-type GBM who underwent F18-FMISO PET imaging before and after the treatment with neoadjuvant bevacizumab. Two patients showing an increase in F18-FMISO accumulation were confirmed with tumor recurrence. These findings suggest that F18-FMISO PET might be useful for monitoring the treatment response to bevacizumab.
Choline-based PET tracers
Choline is an essential molecule participating in the biosynthesis of phosphatidylcholine and an important element of the cell membrane. Several PET radiotracers have been derived from choline, such as C-11 choline, F-18 fluoromethylcholine, F-18 fluorocholine, and F-18 fluoroethyl-choline. C-11 choline and F-18 fluorocholine are phosphorylated intracellularly and then trapped inside cells. The other mechanism of uptake of choline is through disrupted blood–brain barrier.
C-11 choline PET/CT demonstrated a sensitivity of 100% in detecting tumor recurrence in patients who underwent previous treatment of high-grade gliomas. The uptake of C-11 choline was negatively correlated with survival. The patients with higher ratio of C-11 choline tumor uptake/normal brain tissue (T/N) uptake had shorter OS and shorter PFS.
The uptake of F18-fluoromethylcholine PET was demonstrated to distinguish glioblastomas (WHO IV) from grade II/III gliomas ( Fig. 6 ). A study utilized F-18-fluoromethylcholine PET to evaluate the treatment response in patients with GBM and employed quantitative analysis with parameters including the standardized uptake value mean (SUVmean), the MTV, and the MTV × SUVmean. This study showed that F-18 fluoromethylcholine PET could predict treatment response in patients treated with concomitant TMZ and radiation therapy, with a sensitivity of 100% using the MTV × SUVmean.

Related posts:
 Metabolic Brain PET Connectivity
Movement Disorders and Its Variants
Metabolic Brain PET Connectivity
Movement Disorders and Its Variants
 A Brief History and the Use of PET in the Diagnosis and Management of Schizophrenia
A Brief History and the Use of PET in the Diagnosis and Management of Schizophrenia
 Brain PET Imaging in the Presurgical Evaluation of Drug-Resistant Focal Epilepsy
Brain PET Imaging in the Presurgical Evaluation of Drug-Resistant Focal Epilepsy
 Clinical Applications of PET Imaging in Alzheimer’s Disease
Brain Tumor Assessment
Clinical Applications of PET Imaging in Alzheimer’s Disease
Brain Tumor Assessment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


