Tumors of the Cranial and Paraspinal Nerves
Overview
Tumors of the cranial and paraspinal nerves are usually benign, slow-growing neoplasms composed of one or more elements of a nerve cell (Schwann cell, perineural cells, fibroblasts, mast cells, ganglion cells, myxoid/collagenous matrix, and axons). The most common nerve tumor is schwannoma in the general population and in the setting of neurofibromatosis type 2; neurofibromas including plexiform subtype are most commonly seen in the setting of neurofibromatosis type 1.
|
Schwannoma
Definition: Schwannoma is a globular, circumscribed, and encapsulated benign nerve sheath tumor composed of well-differentiated Schwann cells and comprise three main types: conventional, cellular, and plexiform.
Epidemiology: This is the most common peripheral nerve neoplasm, often solitary (90%) but can be multiple in the setting of neurofibromatosis type 2 (4%). It accounts for 8% of all intracranial tumors, 85% of cerebellopontine angle tumors, and 30% of spinal nerve root tumors. No gender predilection has been noted.
Affected age group: Patients of any age are affected, but this tumor is distinctly rare in the pediatric age group. Cerebral intraparenchymal schwannomas are more common in the younger age group, with male dominance.
Molecular and genetic profile: Multiple schwannomas often occur in the setting of two tumor syndromes: neurofibromatosis 2 (NF2) and schwannomatosis. A mosaic pattern of SMARCB1 (INI1) expression is seen in 93% of familial schwannomatosis, 55% of sporadic schwannomatosis, 83% of NF2-associated schwannomas, and only 5% of solitary, sporadic schwannomas.
Clinical features and standard therapy: Clinical presentation depends on the location and type of involved nerve, and incidental detection is common, especially in the peripherally situated schwannomas. Patients with schwannoma involving cranial nerves, such as vestibulocochlear nerve or trigeminal nerve, may present with insidious onset of hearing loss or trigeminal neuralgia, respectively. If resected completely, schwannomas usually do not recur; however, incomplete resection can lead to slow regrowth. Radiation therapy, including ablative radiotherapy such as gamma knife radiosurgery and cyberknife radiotherapy, has been used to treat residual tumors or tumors not amenable to surgery. There is no effective chemotherapy but bevacizumab has been used with mixed response.
Imaging
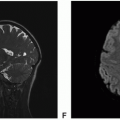
 Figure 8.1. Imaging of right vestibular schwannoma. A. Axial T2: Heterogeneous hypointense mass in the right internal auditory canal and cerebellopontine angle cistern. B. Axial FIESTA: Homogeneous hypointense mass. C. Axial diffusion-weighted imaging (DWI): Heterogeneous isointense mass. D. Axial T1 precontrast: Heterogeneous isointense mass. E. Axial T1 postcontrast: Heterogeneous but avidly enhancing mass. F. Coronal T1 postcontrast: Heterogeneous but avidly enhancing mass. |
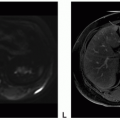
 Figure 8.2. Imaging of left vestibular schwannoma. A. Axial T2: Heterogeneous hyperintense mass in the left IAC and CP angle cistern. B. Axial DWI: Heterogeneous isointense mass. C. Axial apparent diffusion coefficient (ADC): Heterogeneous hyperintense mass. D. Axial T1 precontrast: Hypointense mass. E. Axial T1 postcontrast: Heterogeneous and avidly enhancing mass. F. Coronal T1 postcontrast: Heterogeneous and avidly enhancing mass-dominant component in CP angle and smaller component in the left internal auditory canal (IAC) (arrow). |
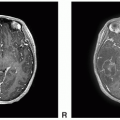
 Figure 8.3. Imaging of vestibular or cochlear schwannomas, 12 differentpatients, axial T1 postcontrast images. A. Left vestibular schwannoma involving vestibule and lateral semicircular canal (arrow). B. Right intracanalicular schwannoma. C. Left cochlear schwannoma (arrow). D. NF type 2 patient: Bilateral internal auditory canal schwannomas (small arrows) and bilateral petrous face meningiomas (long arrows). E. Right IAC and cerebellopontine angle cistern vestibular schwannoma. F. Left IAC and cerebellopontine angle cistern vestibular schwannoma. |
 Figure 8.3. (continued) G. Left IAC and large cerebellopontine angle cistern vestibular schwannoma. H. NF type 2 patient: Left IAC and large cerebellopontine angle cistern vestibular schwannoma, left Meckel’s cave trigeminal schwannoma, and right intracanalicular vestibular schwannoma. I. Left IAC and CP angle vestibular schwannoma with anterior extension (arrow). J. Lobular contour solid enhancing mass in the right CP angle. K. Large heterogeneous, mostly solid left CP angle mass with peripheral (long arrows) and central (short arrows) cystic changes. L. Large heterogeneous, mostly cystic left CP angle mass with internal septations. |
 Figure 8.4. Imaging of facial nerve schwannoma. A-C. Axial (A) and sagittal T2 (B,C): Isointense expansile mass (arrows) in the right geniculate ganglion. D-F. Axial T1 postcontrast: Avid enhancement within the mass. |
 Figure 8.4. (continued) G-I. Coronal T1 postcontrast: Avid enhancement within the mass. J-L. Sagittal T1 postcontrast: Avid enhancement within the mass.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|