Abstract
Objective
Ultrasound bone maturity indexes were used to assess whether children had reached their final height.
Methods
The follow-up study was performed between January 2022 and August 2024. Ultrasound bone maturity indexes, including the ossification ratio of the radius, ulna, and femur, and skeletal maturity score (SMS, the sum of the ossification ratio of the above three bones multiplied by 100), were collected from medical records, along with the children’s age and height. The children were followed up to ascertain the annual increase in height during the 2 years before and after the ultrasound bone age assessment. Children were grouped according to whether they had reached their final height. The diagnostic performance (area under the curve, AUC) of ultrasound bone maturity indexes in assessing whether the children had reached their final height was confirmed.
Results
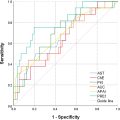
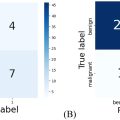
A total of 120 children (60 boys) with a mean age of 15.0 ± 1.7 years for boys and 14.1 ± 2.0 years for girls were included. At the attainment of final height, the mean values of radial, ulnar, and femoral ossification ratios, as well as the SMS, were 90%, 84%, 98%, and 271 in boys and 86%, 83%, 98%, and 267 in girls, respectively. Ultrasound bone maturity indexes were able to assess whether children had reached their final height, with the highest AUC for SMS of 0.99 (95% CI: 0.97, 1.01, cutoff value, 256) in boys and 0.95 (95% CI: 0.90, 1.00, cutoff value, 260) in girls.
Conclusion
A child’s height stops increasing before the ossification ratios of the bones reach 100%. Ultrasound bone maturity indexes, especially SMS, demonstrate high diagnostic performance in determining whether children have reached their final height.
Introduction
Whether children have reached their final height is a common concern for parents and serves as an important reference for pediatric endocrinologists when making clinical decisions about children’s growth and development [ ].
According to Li’s study [ ], Chinese boys were close to their adult height after 16.0 years of age, while girls were close to theirs after 15.0 years of age. However, due to factors such as genetics, pathology, environment, and others, it is not accurate to determine whether children have reached their final height based solely on age.
Bone age is an indicator of skeletal growth and development in children and is traditionally assessed using X-rays of the hand and wrist. Previous studies [ , ] have predicted final height based on X-ray bone age, often using epiphyseal and metaphyseal fusion as the endpoint for cessation of skeletal growth. In 1994, Smith et al. [ ] reported the case of a 28-year-old estrogen-resistant adult male with a mutation in the estrogen receptor gene. X-rays of his left hand, wrist, and knee revealed that the growth plates remained open, yet he had ceased growing in height. Therefore, it is inaccurate to use the closure of the growth plates on X-rays to determine whether final height has been reached. The patient had stopped growing before the growth plates closed. While, except for growth plate closure, there is a lack of a quantitative assessment index for judging whether bone growth has stopped.
MRI can directly visualize the status of growth plates, and diffusion tensor imaging (DTI) can reveal the microstructure of the growth plate and epiphysis in children [ ]. However, there is a lack of studies using DTI to assess children’s final height. What’s more, MRI is time-consuming and expensive, limiting its widespread use in the assessment of children’s growth and development.
Recent studies have demonstrated that conventional ultrasound can visualize the ossification center and epiphyseal cartilage at the ends of long bones and measure their heights [ ]. The ratio of the height of the ossification center to the height of the epiphyseal cartilage, known as the ossification ratio, enables the quantitative assessment of skeletal growth and development. The process of bone maturation is the increase of the ossification ratio from 0% to 100% [ ]. SMS (the sum of the ossification ratios of the radius, ulna, and femur multiplied by 100%) may reflect bone maturation in the long bones of children. However, there are no reported studies on the relationship between such ultrasound-based maturity indexes and the final height of children.
We speculate that the ossification ratio measured by ultrasound may serve as an indicator of whether a child has reached their final height. We will measure the ossification ratios of the radius, ulna, and femur, as well as the SMS, in children using conventional ultrasound to evaluate the diagnostic value of the ultrasound-based maturity indexes in assessing final height attainment.
Materials and methods
Our study was performed from January 2022 to August 2024 as part of the ultrasound bone age project, a follow-up to the original study. The ultrasound bone age project was a prospective study conducted in 2020 that assessed the bone age of children by conventional ultrasound. The study received approval from the local institutional review board and was registered on the Chinese clinical trial registry website ( http://www.chictr.org.cn , No. ChiCTR1900027917). Informed consent was obtained from the parents or guardians of all children included in the study.
Study participants
In this study, medical records of children who underwent ultrasound bone age assessment as part of the ultrasound bone age project were analyzed. The participants were screened according to the following inclusion and exclusion criteria.
The inclusion criteria for the study population were an age between 11.0 and 18.0 years at the time of the examination. The exclusion criteria included: (i) pathological changes in the wrist and knee joints, such as tumors and trauma; (ii) absence of height measurements at the time of ultrasound examination; and (iii) lack of follow-up data on current height. The protocol used in this study is shown in Figure 1 .

Demographics, ultrasound images, and follow-up
Demographic information, including name, gender, height, date of birth, and date of examination, was collected from all participants.
Ultrasound examinations were performed using a Philips EPIQ ultrasound machine equipped with an eL18-4 high-frequency linear array probe. All image acquisitions and calculations of ossification ratio were performed independently by the same sonographer, who had more than twenty years of experience. All children underwent ultrasound examinations of the left radius, ulna, and knee. The ossification ratios of the radius, ulna, and femur, as well as the SMS, were calculated. The methods and procedures for the ultrasound examination and the calculation of the ossification ratio were performed according to the protocol described in a previous article [ ] ( Fig. 2 ). The heights of the children were collected from medical records and through telephone callbacks to clarify the change in height over the 2 years before and after the time when the children underwent the ultrasound examination. Guardians were trained on the method of height measurement during the follow-up visit. Specifically, a slight upward pressure was applied under the child’s mastoid process to stretch the child to their maximum height before measurement [ ].

Diagnostic performances
A height gain of less than 1 cm for one consecutive year was considered indicative of reaching final adult height [ ]. The children were grouped according to whether they had reached their final height. The diagnostic performance of ultrasound parameters in confirming that the children had reached their final height was assessed using the area under the ROC curve (AUC), sensitivity, and specificity. For AUC values, 0–0.5, 0.5–0.7, 0.7–0.9, 0.9–1, and 1 were considered to represent no, low, intermediate, high, and full diagnostic power, respectively [ ].
Statistical analysis
All data were analyzed using SPSS 26.0 (IBM). Continuous variables are presented as mean ± standard deviation (SD). Differences between groups were analyzed using Student’s t test. Differences in AUC between groups were analyzed using the Delong test. All statistical tests were two-sided, and a p value < 0.05 was considered to indicate a statistically significant difference.
Results
A total of 120 children (60 boys) were eventually enrolled in the study. The mean age at the time of ultrasound examination was 15.0 ± 1.7 years (range: 11.5–17.9 years) for boys and 14.1 ± 2.0 years (range: 11.4–17.9 years) for girls.
Ultrasound ossification ratio and SMS in each group
A total of 53 children reached their final height. Twenty-two of them reached their final height more than one year before the time of ultrasound measurement. The ossification ratio of each bone was 100%. The age of the 22 children was 17.2 ± 0.7 years in boys and 16.9 ± 0.7 years in girls. The remaining 31 children reached their final height within 1 year before or after the ultrasound examination. The age, height, and ultrasound bone maturity indexes are listed in Table 1 . The ossification ratio of the bones in 11 children (5 boys) did not reach 100% by the time they reached their final height. The ossification ratio of the femurs in these 11 children was 93 ± 2% ( Fig. 3 ). No significant differences were found between boys and girls in the ossification ratios of the ulna, femur, and SMS when they reached their final height ( p > 0.05).
| Boys (n = 14) | Girl (n = 17) | p | |
|---|---|---|---|
| Age (years) | 16.1 ± 1.2 (95% CI: 15.4, 16.8) | 14.8 ± 1.0 (95% CI: 14.3, 15.4) | 0.003 |
| Height (cm) | 173.4 ± 7.5 (95% CI: 169.0, 177.7) | 160.8 ± 7.0 (95% CI: 157.2, 164.4) | 0.000 |
| Radius (%) | 90 ± 5 (95% CI: 87, 93) | 86 ± 4 (95% CI: 84, 88) | 0.019 |
| Ulna (%) | 84 ± 10 (95% CI: 78, 89) | 83 ± 13 (95% CI: 76, 90) | 0.905 |
| Femur (%) | 98 ± 4 (95% CI: 96, 100) | 98 ± 3 (95% CI: 96, 99) | 0.958 |
| SMS | 271 ± 15 (95% CI: 263, 280) | 267 ± 16 (95% CI: 259, 275) | 0.416 |

Related posts:
 Quantitative Analysis of Contrast-Enhanced Ultrasound Images of Brain-Dead Donor Livers: Prediction of Early Allograft Dysfunction
Quantitative Analysis of Contrast-Enhanced Ultrasound Images of Brain-Dead Donor Livers: Prediction of Early Allograft Dysfunction
 Safety of Shear Wave Elastography as Evidenced From Carotid Artery Strain and Strain Rate Induced by Acoustic Radiation Force Impulse and Arterial Pulsations
Safety of Shear Wave Elastography as Evidenced From Carotid Artery Strain and Strain Rate Induced by Acoustic Radiation Force Impulse and Arterial Pulsations
 Ultrasound Shear Wave Elastography and Shear Wave Dispersion: Correlation with Histopathological Changes in Autoimmune Hepatitis Patients
Ultrasound Shear Wave Elastography and Shear Wave Dispersion: Correlation with Histopathological Changes in Autoimmune Hepatitis Patients
 Diagnosis of Salivary Gland Tumors Using Ultrasound Radiomics
Diagnosis of Salivary Gland Tumors Using Ultrasound Radiomics
 Empirical Model of Focused Ultrasound-Mediated Treatment for Chemotherapy Delivery to Brain Tumors
Empirical Model of Focused Ultrasound-Mediated Treatment for Chemotherapy Delivery to Brain Tumors
 High-Frequency Ultrasound Characterization of Periodontal Soft Tissues Pre- and Post-Bacterial Inoculation
High-Frequency Ultrasound Characterization of Periodontal Soft Tissues Pre- and Post-Bacterial Inoculation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


