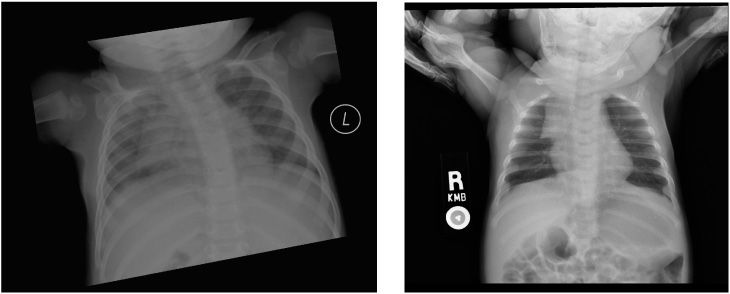
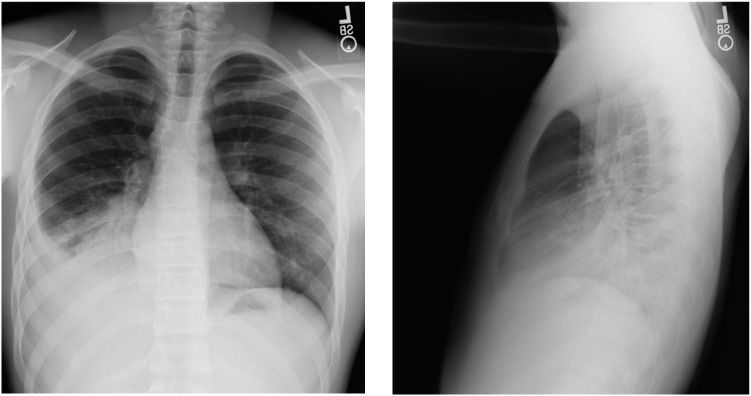
7-month-old female with cough
1. Describe the findings.
2. Where is the thymus anatomically located?
3. What is the thymic sail sign?
4. What is the thymic wave sign?
5. How and when is the spinnaker sign formed?
Normal thymus 682
Case ranking/difficulty: | Category: Thorax |
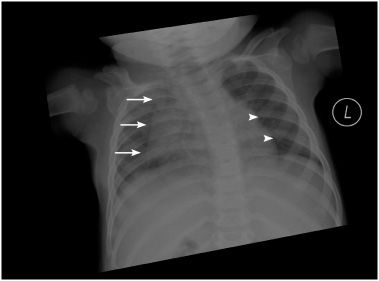
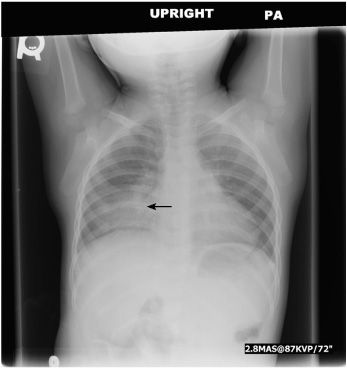
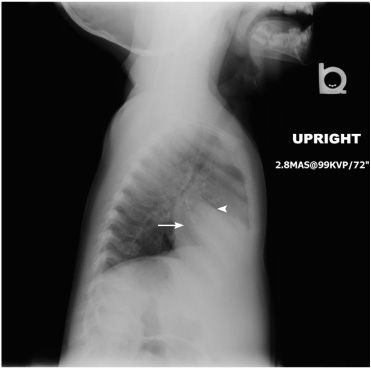
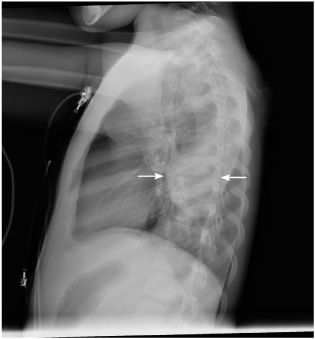
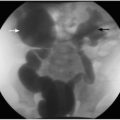
Frontal radiograph of the chest demonstrates the sail sign of normal thymus appearance (arrows). The thymus has a wavy appearance that is noted between the ribs (arrowheads).
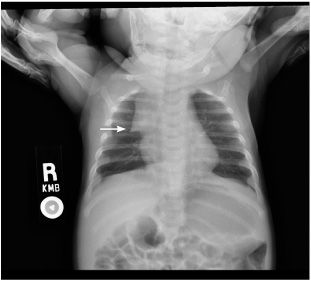
Frontal view of the chest of another 2-month-old male represents the sail sign (arrow).
Answers
1. The sail sign and the wave sign are seen consistent with normal thymus in an infant.
2. The thymus occupies the anterior and superior mediastinum, located behind the sternum in the midline. In infancy, the upper border of the thymus extends almost to the thyroid gland in the neck and the lower margin overlaps the upper part of the heart, occasionally extending as far as the diaphragm.
3. The sail sign seen in 8.8% of children describes a triangular soft tissue density forming either the right, left, or both mediastinal borders.
4. The wave sign is normal indentation of the thymus laterally by the adjacent anterior ribs. The thymic notch is an indentation seen at the junction of the thymic and the cardiac outlines.
5. The spinnaker or angels wing sign describes the elevation of the thymus in the presence of pneumomediastinum.
Suggested Readings
Correia-Pinto J, Henriques-Coelho T. Images in clinical medicine. Neonatal pneumomediastinum and the spinnaker-sail sign. N Engl J Med. 2010;363(22):2145.
Han DH. Thymic sail sign: unique to paediatric chest radiographs? Pediatr Radiol. 2010;40(3):375-376.
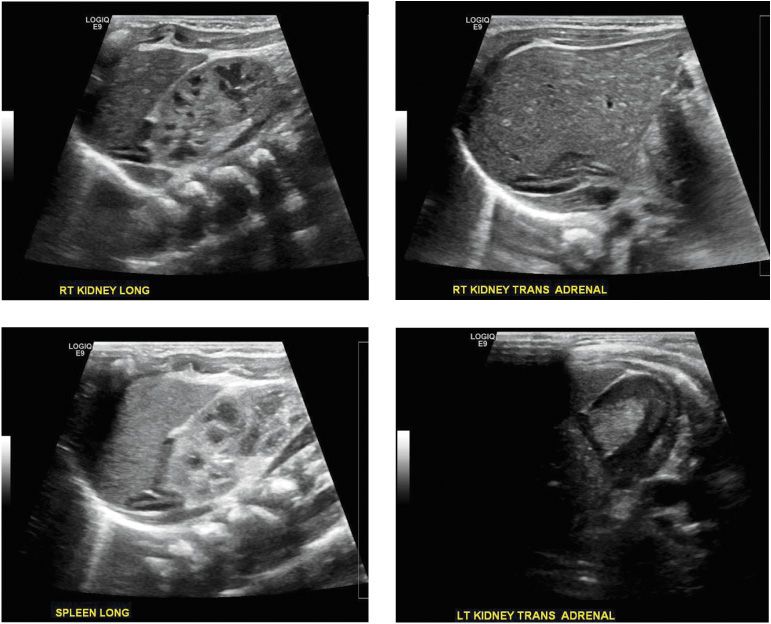
1-day-old male who underwent abdominal sonographic study
1. What are the principal landmarks for visualization of the right adrenal gland in neonatal ultrasound?
2. What are the principal landmarks for visualization of the left adrenal gland in neonatal ultrasound?
3. Where is the upper pole of the left kidney normally located in relation to the left adrenal gland?
4. How does the cortex of the normal adrenal glands appear in neonatal ultrasound?
5. How does the central medulla of the normal adrenal glands appear in neonatal ultrasound?
Neonatal adrenal gland, normal 641
Case ranking/difficulty: | Category: Abdomen |

Longitudinal sonogram of the right upper quadrant of the abdomen demonstrates normal appearance of the right adrenal gland (arrow), normal right kidney (arrowhead), and liver (L).

Transverse sonogram of the right upper quadrant of the abdomen demonstrates normal appearance of the right adrenal gland (arrow) and normal liver (L).

Longitudinal sonogram of the left upper quadrant of the abdomen demonstrates normal appearance of the left adrenal gland (arrow), normal left kidney (arrowhead), and spleen (S).

Transverse sonogram of the left upper quadrant of the abdomen demonstrates normal appearance of the left adrenal gland (arrow) and normal appearance of the edge of the spleen (asterisk).
Answers
1. The right adrenal gland is supramedial to the right kidney. The right kidney is posterolateral to the inferior vena cava.
2. The key landmarks are the aorta medially, the left inferior crus of the diaphragm, and the lower pole of the spleen or upper renal pole laterally.
3. The upper pole of the left kidney is normally located laterally and inferiorly in relation to the left adrenal gland.
4. The cortex of the normal adrenal glands is hypoechoic in neonatal ultrasound.
5. The central medulla of the normal adrenal glands is hyperechoic in neonatal ultrasound.
Suggested Readings
Oppenheimer DA, Carroll BA, S Yousem S. Sonography of the normal neonatal adrenal gland. Radiology. 1983;146:157-160.
Prokop M, Galanski M, Schaefer-Prokop C. Spiral and multislice computed tomography of the body. George Thieme Verlag. 2003. ISBN:0865778701.
Yeh HC. Sonography of the adrenal glands: normal glands and small masses. AJR Am J Roentgenol. 1980;135(6):1167-1177.
Healthy 15-year-old male with fever and cough
1. What are the findings in the frontal view of the chest?
2. What are the findings in the lateral view of the chest?
3. In which lobe is the opacity seen in the images located?
4. What is the most likely underlying diagnosis?
5. What is the etiology of the disease?
Right lower lobe pneumonia 148
Case ranking/difficulty: | Category: Thorax |
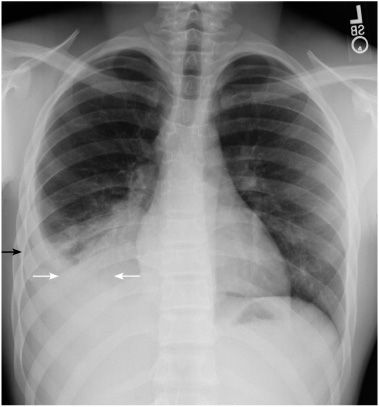
Frontal radiograph of the chest reveals opacity of the right lower lobe. There is silhouetting of the right hemidiaphragm (white arrows). There is obscuration of the right costophrenic sulcus (black arrow) representing right-sided pleural effusion.
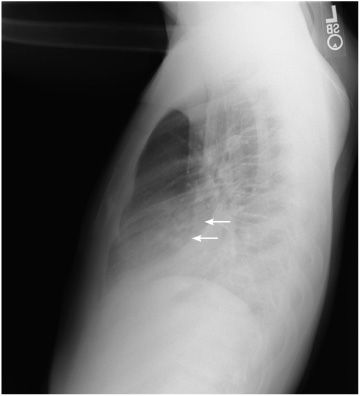
Lateral radiograph of the chest reveals opacity of the posterior lower lung zone, posterior to the major fissure (white arrows). In comparison to the frontal view, it represents right lower lobe air-space disease.
Answers
1. Findings are silhouetting of the right hemidiaphragm and obscuration of the right costophrenic sulcus.
2. Findings are opacity in the lower lung zone posterior to the major fissure and silhouetting of the posterior aspect of the diaphragm.
3. The opacity seen in the images is located in the right lower lobe.
4. The most likely diagnosis is community-acquired pneumonia.
5. The etiology is infectious.
Suggested Readings
Arnold FW, Ramirez JA, McDonald LC, Xia EL. Hospitalization for community-acquired pneumonia: the pneumonia severity index vs clinical judgment. Chest. 2003;124(1):121-124.
Claudius I, Baraff LJ. Pediatric emergencies associated with fever. Emerg Med Clin North Am. 2010;28(1):67-84, vii-viii.
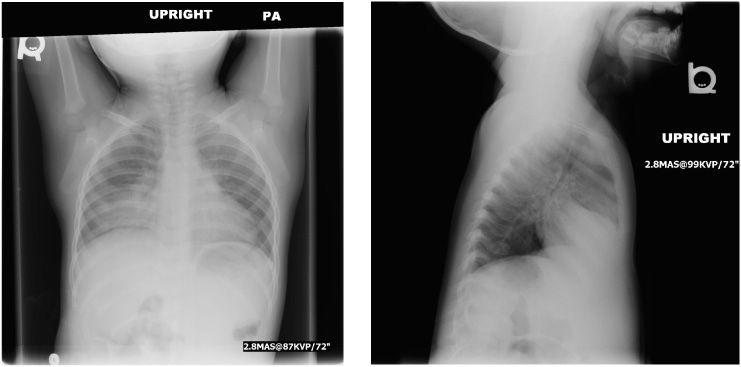
3-year-old female with fever and cough
1. How are patients with this entity present clinically?
2. What are the borders of the opacity in the lateral view of the chest?
3. Why is the right heart border in the frontal view of the chest obscured?
4. What is the most common organism causing this entity?
5. What is the treatment option?
Right middle lobe pneumonia 93
Case ranking/difficulty: | Category: Thorax |
Frontal radiograph of the chest shows opacity in the medial aspect of the right lower lung zone with the silhouette sign involving the right heart border (arrow) that indicates a process in the right middle lobe. The entire right hemi-diaphragm is seen, meaning that the right lower lobe is not involved.
Lateral radiograph of the chest shows consolidation that appears as a wedge-shaped density overlying the heart, bordered superiorly by the minor fissure (arrowhead) and inferiorly by the major fissure (arrow).
Answers
1. Clinical presentation includes fever, cough, wheezing, and tachypnea.
2. The opacity is bordered by the minor fissure superiorly and major fissure inferiorly.
3. In the frontal view, the right heart border is obscured by the right middle lobe opacity.
4. Most likely etiology is gram-positive bacteria such as Streptococcus pneumoniae.
5. Treatment is antibiotics.
Suggested Readings
Dees SC, Spock A. Right middle lobe syndrome in children. JAMA. 1966;197(1):8-14.
Lutfiyya MN, Henley E, Chang LF. Diagnosis and treatment of community-acquired pneumonia. Am Fam Physician. 2006;73:442-450.
10-year-old male with fever and cough
1. Describe the findings.
2. What may be the complications of such entity?
3. What constituents can be found in exudate of this entity?
4. What are the most common organisms causing community-acquired pneumonia?
5. What are the most common organisms causing pneumonia in the neonatal period?
Left lower lobe pneumonia 429
Case ranking/difficulty: | Category: Thorax |
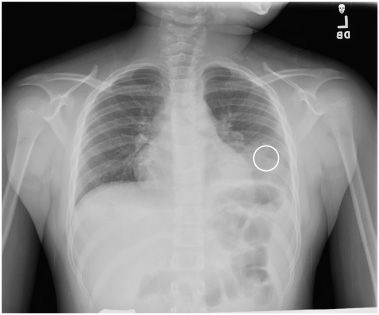
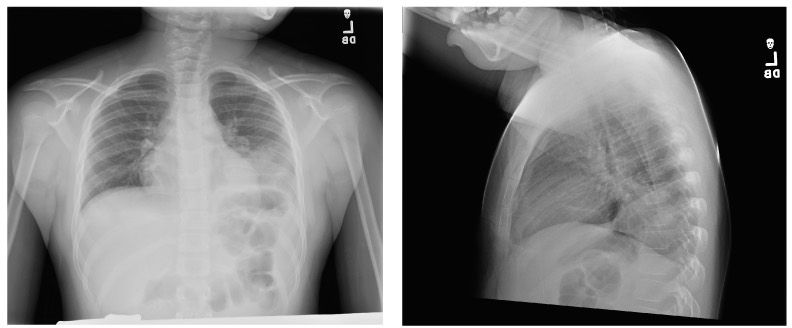
Frontal radiograph of the chest reveals opacity of the left lower lobe (circle). Compared to the upper-left lung zone there is density in the lateral aspect of the lower lung zone. The left heart border is preserved. There is obscuration of the left hemidiaphragm.

Lateral radiograph of the chest reveals a retrocardiac density in the posterior lower lung zone (circle). Normally posteriorly as we look caudally, the lung should become more lucent. In this image, the lung becomes more dense posteriorly.
Answers
1. There is retrocardiac opacity. In lateral view, there is density in the lower posterior lung zone. There is loss of the left hemidiaphragm (“silhouette sign”) and preservation of the left heart border, indicating involvement of the left lower lobe and sparing of the lingula of the left upper lobe.
2. Complication of pneumonia may include pulmonary failure, pleural effusion, pneumatocele, and necrotizing pneumonitis.
3. In the exudate due to pneumonia, there are proteins such as fibrin, and pus is found with white blood cells.
4. The most common organisms causing community-acquired pneumonias are Chlamydia pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, Streptococcus pneumoniae, and a variety of respiratory viruses.
5. The most common organisms causing pneumonia in the neonatal period are Group B Streptococcus, Listeria monocytogenes, Klebsiella pneumoniae, and Escherichia coli.
Suggested Reading
Thompson BH, Berbaum KS, George MJ, Ely JW. Identifying left lower lobe pneumonia at chest radiography: performance of family practice residents before and after a didactic session. Acad Radiol. 1998;5(5):324-328.
7-year-old male with cough, fever, and leukocytosis
1. What are the findings?
2. What is the differential diagnosis?
3. What is the underlying pathophysiology of this entity?
4. What is the most causative agent of this entity?
5. What should be the appropriate management?
Round pneumonia 1659
Case ranking/difficulty: | Category: Thorax |

Frontal view of chest radiograph reveals round opacity in the superior segment of the left lower lobe (arrows).
Lateral view of chest radiograph reveals round opacity in the superior segment of the left lower lobe (arrows).
Answers
1. There is a rounded opacity in the superior segment of the left lower lobe.
2. Posterior mediastinal mass, round pneumonia, and loculated pleural fluid.
3. The pathophysiology of round pneumonia is the absence of collateral air communicating pathways in children (ie, pores of Kohn, canals of Lambert), which limit spread of infection.
4. Round pneumonia is caused by bacterial infection, with Streptococcus pneumoniae being the most common causative organism.
5. Ultrasound can help confirm the diagnosis of round pneumonia by demonstration of sonographic air bronchogram as linear branching echogenic structures within the lesion. Repeat radiograph in 1 to 2 weeks after antibiotics treatment would show improvement in lung opacity. CT scan has much higher radiation and should be avoided.
Suggested Readings
Kim YW, Donnelly LF. Round pneumonia: imaging findings in a large series of children. Pediatr Radiol. 2007;37(12):1235-1240.
Restrepo R, Palani R, Matapathi UM, Wu YY. Imaging of round pneumonia and mimics in children. Pediatr Radiol. 2010;40(12):1931-1940.
Shah CC, Greenberg SB. Pediatric chest. In: Rumack CM, Wilson SR, eds. Diagnostic Ultrasound. 4th ed. Philadelphia, PA: Elsevier; 2011:1768-1799.
15-year-old male with chest deformity
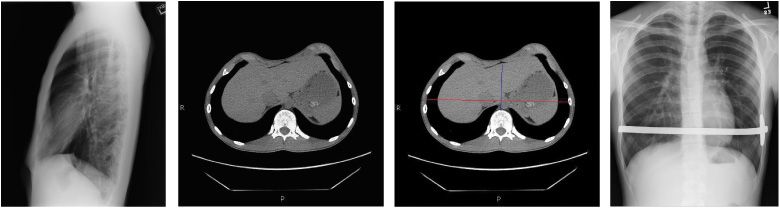
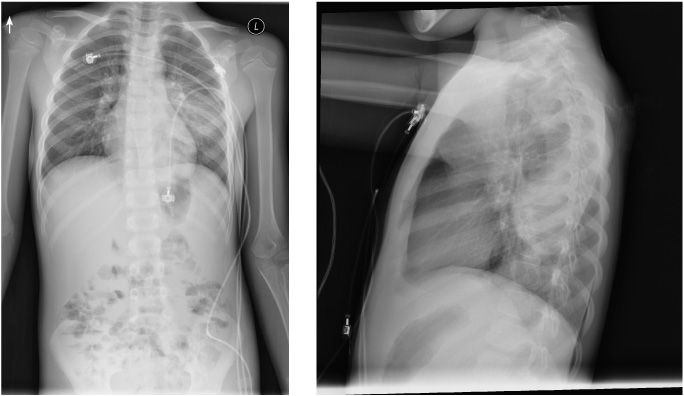
1. Describe the findings of the first three figures.
2. Describe the findings of the last figure.
3. What is the Haller index?
4. What are the complications of this entity?
5. What are the treatment options?
Pectus excavatum 661
Case ranking/difficulty: | Category: Thorax |

Lateral radiograph of the chest demonstrates concave appearance of the lower anterior chest wall (arrow).

Non-contrast CT of the chest demonstrates concave appearance of the lower anterior chest wall (arrow). The level of the CT is the narrowest antero-posterior diameter.

Non-contrast CT of the chest demonstrates concave appearance of the lower anterior chest wall (arrow). The level of the CT is the narrowest antero-posterior diameter. The blue line is a line drawn to measure the narrowest frontal diameter of the inner chest. The red line was drawn to measure the inner transverse diameter of the chest at the level of the narrowest antero-posterior diameter. These measurements were performed for calculation of Haller index.
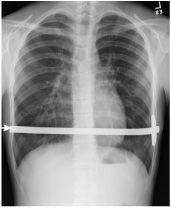
Frontal view of the chest following surgical correction demonstrates the pectus bar (arrow).
Answers
1. There is concave appearance of the lower anterior chest wall due to a decrease in the antero-posterior diameter of the lower chest.
2. The bar seen in the lower chest was placed during the surgical correction of pectus excavatum. This is the Lorenz pectus bar, which is a convex transverse bar placed under the anterior chest wall.
3. Haller index is derived by dividing the transverse chest diameter by the antero-posterior diameter. This is done at the narrowest antero-posterior diameter of the chest. An index of more than 3.2 has been correlated with a severe deformity that requires surgery.
4. Depending on the severity, pectus excavatum can impair cardiac and respiratory function and cause pain in the chest and back.
5. Treatment is performed with the Nuss procedure and with the placement of a Lorenz pectus bar.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


