• The iliofemoral ligament is the strongest ligament of the hip joint. It is a thickening of the hip joint capsule (intrinsic ligament), as are the ischiofemoral and pubofemoral ligaments. • If there is clinical suspicion of a labral tear, the preferred imaging procedure is an MR arthrogram of the hip. • A small branch of the obturator artery (acetabular) passes through the ligament of the head of the femur (ligamentum teres) to supply the femoral head, but this branch is usually too small to prevent necrosis if the circumflex arteries are torn. • In cases of avascular necrosis, the femoral head is removed and a prosthetic hip joint is surgically implanted. • The profunda femoris artery (deep femoral artery) supplies the muscles of the posterior thigh. • The iliopectineal (iliopsoas) bursa allows the iliopsoas muscle/tendon to move freely over the hip joint as it flexes the thigh. (In the case shown here the normally collapsed bursa is visible because of excess fluid.) • The iliopsoas tendon (common tendon of iliacus and psoas major muscles) inserts onto the lesser trochanter. • Grade 1 muscle injury is a strain of the muscle without architectural disruption. In Grade 2 muscle injury there is more clearly visible disruption of muscle fibers with hemorrhage. Grade 3 muscle injury is characterized by a complete disruption of the muscle. • All four parts of the quadriceps femoris muscle group are innervated by the femoral nerve, which is composed of the dorsal divisions of the ventral rami of L2-L4 spinal segments. • The great saphenous vein has been the vessel of choice for coronary artery grafting for many years, although other vessels (e.g., radial, internal thoracic arteries) are now often used. If the vein is used it must be positioned so that the valves do not impede blood flow. • Once the popliteal vein passes through the adductor hiatus in the adductor magnus muscle it becomes the femoral vein. • Clinically suspected pulmonary thromboembolic disease is usually evaluated by a pulmonary CT angiogram to identify or rule out pulmonary emboli. The scan protocol may include a low-dose CT scan of the lower limbs, usually done approximately 2 minutes after the IV contrast injection for the pulmonary artery study. This additional scan may demonstrate popliteal and femoral vein thrombi. • The adductor magnus muscle is actually two muscles that are well blended anatomically, but distinct functionally. The superior part is innervated by the obturator nerve and acts with the other adductors in flexing and adducting the femur. The lower part is innervated by the tibial part of the sciatic nerve and acts with the hamstrings as a hip extensor. • The obturator externus muscle covers the external surface of the obturator membrane and is a strong lateral rotator of the femur. • A volume rendered display, such as this image, permits visualization of the posterior relationship between the obturator externus muscle and the femoral neck. • The top image is oriented to the long axis of the sciatic nerve as it courses through the greater sciatic foramen; the nerve, which is isointense with muscle, is surrounded by high-signal perineural fat. • The lower image shows how intragluteal injections placed too far inferiorly and too far medially could injure the sciatic nerve.
Lower Limb





Hip Joint

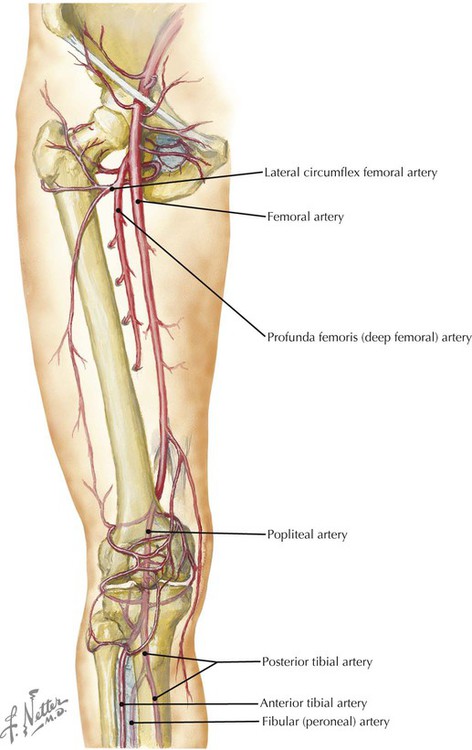
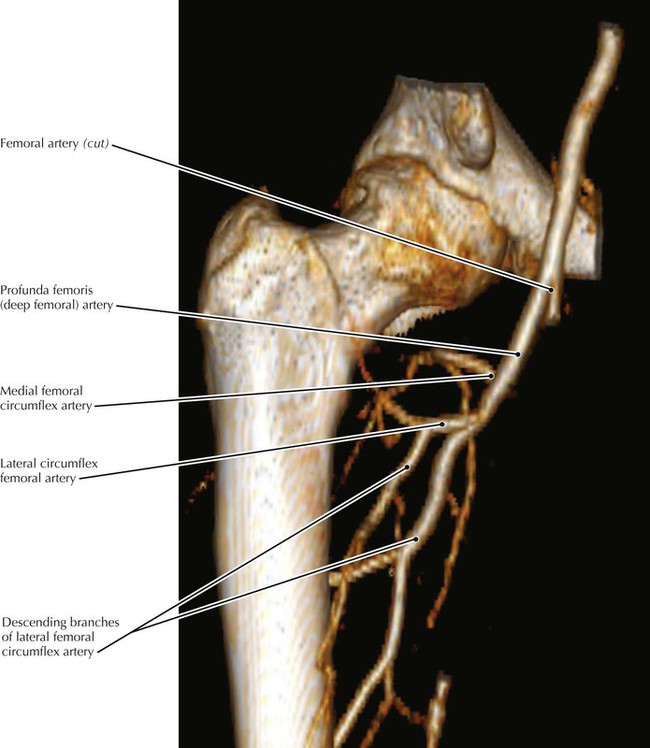
Vasculature of the Femoral Head

Iliopectineal Bursa
Quadriceps Femoris Muscle Group

Deep Anterior Thigh Region


Deep Hip Muscles
Sciatic Nerve


Radiology Key
Fastest Radiology Insight Engine