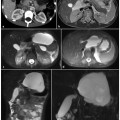
Fig. 1.1
Magnetic resonance imaging findings in a normal pancreas. a Axial T1-weighted in phase image, b axial T2- weighted rapid acquisition with relaxation enhancement (RARE) image, c axial T1-weighted gradient-echo with fat saturation, d axial T2-weighted half-Fourier acquisition single-shot turbo-spin-echo (HASTE) with locator parallel to the body of the pancreas for further magnetic resonance cholangiopancreatography planning
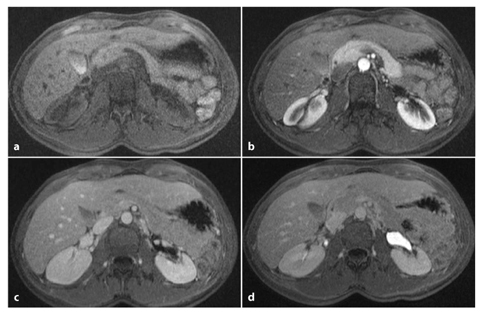
Fig. 1.2
Dynamic magnetic resonance imaging during contrast agent administration: normal pattern. Axial T1-weighted gradient-echo with fat saturation before administration of intravenous constrast agent (a), and during pancreatic (b), portal venous (c) and equilibrium (d) phases
1.3 MRCP Techniques
MRCP techniques use heavily T2-weighted sequences with long echo times to depict the fluid within the biliary ductal system as high signal intensity, while the background signal intensity from liver and other parenchymal organs is suppressed.
There are three main ways to obtain MRCP images (Table 1.1). State-of-the-art MRCP imaging currently uses RARE sequences, and the two typical sequences are: (1) the multislice two-dimensional (2D) fast-spin-echo (FSE)/turbo-spin-echo (TSE) sequence with half-Fourier acquired k-space (single-shot FSE/TSE), where the most commonly used sequence is the T2-weighted 2D half-Fourieracquired single-shot (SS) TSE (HASTE) sequence [7]; and (2) the single-slice thickslab SS-FSE/TSE RARE sequence [8].
Table 1.1
Magnetic resonance cholangiopancreatography: type of sequence and parameters employed
Sequence parameter | SS-FSE | Multislice T2-HASTE | 3D-TSE |
|---|---|---|---|
TR | ∞ | ∞ | Approximately 4 s (depending on patient’s respiratory cycle) |
TE (ms) | 985 | 66–75 | 655 |
FOV (mm) | 350 | 380 | 300 |
Slice thickness (mm) | 60 | 6–8 | 1.3 |
Number of slices | 1 | 36 | 40 |
Matrix | 512×512 | 320×320 | 384×384 |
Time of acquisition | 0.5 s | 2 ( 18) s | 3–5 min |
Respiratory acquisition mode | Breath-hold | Breath-hold | Respiratory gating |
Another approach is 3D MRCP, which uses a high-resolution 3D T2-weighted TSE sequence with an isotropic voxel size and navigator trigger.
1.3.1 Multislice Half-Fourier Acquistion Single-Shot Turbo-Spin-Echo (HASTE)
HASTE sequences have an important role in acquiring MRCP images. HASTE is a highspeed pulse sequence that uses a 90° radio frequency excitation pulse followed by a long series of spin echoes (echo train). The interval between successive echoes is as short as possible. So this is a single-shot approach whereat each echo is individually phase encoded during the very long echo train (e.g., 256) [9].
As a result of its high echo train length, HASTE is particularly appropriate for imaging fluid. The entire 2D image data are acquired in a single echo train by using half-Fourier acquisition. This results in incomplete acquisition of k-space data that fill half of the k-space, while the remaining k-space data are reconstructed by exploiting k-space symmetry. Therefore this technique, which relies on the symmetry of the k-space, permits fast acquisition times. Each slice is acquired after a single excitation pulse and the acquisition time is about 1 s per slice. This advantage makes it possible to use breathhold with excellent motionless MRI [10, 11].
When used in the context of MRCP, HASTE is performed on both axial and coronal planes, with the following parameters: TR 1900 ms, TE 76–66 ms, matrix 320×320, slice thickness 8 mm on axial plane, 6 mm on coronal plane. This sequence permits the acquisition of thin slices (6–8 mm) in combination with better depiction of the surrounding tissue, and it allows a much better anatomical correlation without superimposition of signal-intense structures such as fluid collections, and therefore the sequence is used in all abdominal MR examinations (Fig. 1.3).
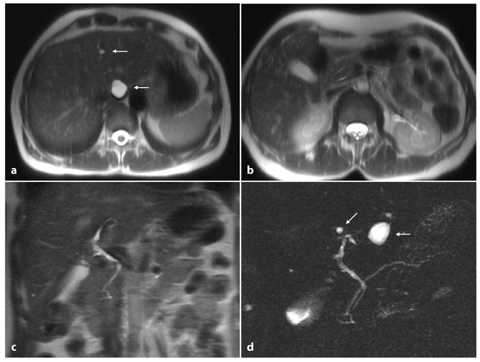
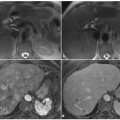
Fig. 1.3
Ductal imaging: biliary tree and pancreatic duct system. Axial T2-weighted half-Fourier acquisition singleshot turbo-spin-echo (HASTE) (a, b), coronal T2-weighted HASTE (c) and magnetic resonance cholangiopancreatography (d) images show a non-dilated intrahepatic biliary tree, common bile duct and main pancreatic duct confluence; multiple hepatic cysts are also evident (arrows)
HASTE is superior to other MRCP sequences in distinguishing structures adjacent to the biliary system and it permits a detailed evaluation of anatomical background for the differentiation of benign and malignant stenosis.
As all the data for one slice are acquired after a single excitation pulse, HASTE allows image acquisition within a few seconds, and this is important in patients who cannot cooperate well. Moreover with HASTE, and also with single thick-slab RARE sequences, we can perform dynamic acquisitions in order to delineate the dynamic filling states of the ampullary region, repeating sequences in the same position after an interval of a few seconds.
The major drawback of HASTE imaging is flow artifact, which manifests itself as a signal loss within the lumen that may mimic endoluminal filling defects. The artifact occurs more frequently in the transverse slice orientation, and it is due to the arterial pulsation of the adjacent hepatic artery.
Some authors suggest the use of a doubleecho HASTE technique with two images calculated per anatomical slice position. This acquires two images per RF excitation: a first image with a relatively short effective TE (75 ms) and a second image with a long effective TE (350 ms). This increases the acquisition time per slice, but it permits excellent visualization of fluid-containing structures and lesions on images with long TE [12].
1.3.2 Thick-Slab Single-Shot Fast- Spin-Echo/Turbo-Spin-Echo Sequence
The thick-slab single-shot (SS) technique is a fast-spin-echo (FSE)/turbo-spin-echo (TSE) sequence based on a 2D SS section in one sin- gle slice with a high slice thickness (30–80 mm) that can be obtained in any plane with a single short breath-hold [7, 10, 11]. The resulting T2-weighted image is similar to projection radiography or ERCP images.
This sequence is characterized by one 90° RF pulse followed by a very long echo train comprising, for example, 256 or more spin echoes. All data are acquired after one single RF excitation pulse within one single echo train; every single spin echo is separately phase encoded [13].
The echo time usually exceeds 635 ms (985 ms in our clinical practice) and, thus, practically all the signal from tissue apart from the stationary fluids is suppressed. The acquisition time of one single measurement is in the order of 1 s. In order to include the pancreaticobiliary system in its entire extent within one single planar projection, the measurement slab usually has a thickness of 60 mm.
Acquisition parameters that we commonly use for SS-FSE MRCP are TR 4500 ms, TE 985 ms, ETL 256, matrix 512×512, 60 mm slice.
Different projections are acquired, and these are angulated along the relevant anatomical structures. These are recognized on a previously performed axial T2-weighted HASTE. The technologist is instructed to obtain radial slabs centered on the pancreatic head (Fig. 1.4) and a few slabs (generally three) oriented in a straight coronal plane and parallel to the pancreatic tail (Fig. 1.5). Additional slabs are obtained at the discretion of the technologist.

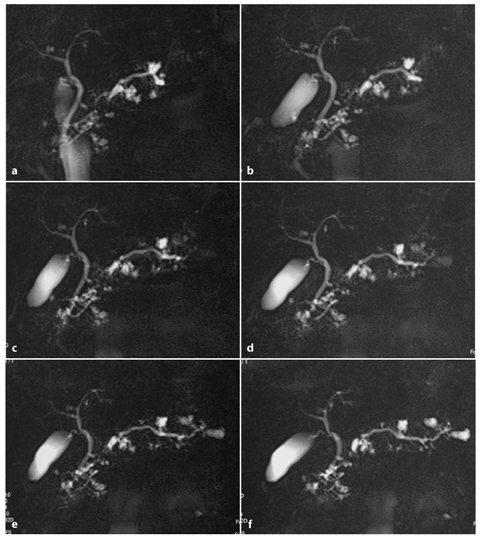
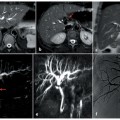
Fig. 1.4
a Positioning of radial magnetic resonance cholangiopancreatography (MRCP) on a previously performed axial T2-weighted half-Fourier acquisition single-shot turbo-spin-echo (HASTE). b–f Resulting MRCP images centered radially to the pancreatic head
Fig. 1.5
Multiple oriented coronal and coronal-oblique magnetic resonance cholangiopancreatography images prescribed parallel to the pancreatic head (a–c) and to the tail (d–f). Images show multiple side-branch intraductal papillary mucinous neoplasms along the whole pancreatic parenchyma
The major advantage of the thick-slab SS RARE sequence is the ultrafast image acquisition, in the order of 1 s, and the fact that no further post-processing is required. Imaging can be repeated during consecutive breathholding episodes using a different slice position and orientation in order to obtain visualization of the entire biliary tree and pancreatic ductal system. Also, in the case of suspected biliary obstruction, kinematic imaging can be performed by repeating the acquisition without changing the parameters for slice position and slice orientation. Hence, for severely ill patients with limited respiratory capacities, the RARE sequence may be the only imaging technique to obtain sufficient image quality with the least artifacts.
Because of the short acquisition time and there being no need for post-processing, interpretation is available immediately. In addition, the short acquisition time allows the technologist to obtain sequential acquisitions, each during a single breath-hold after stimulation with secretin (dynamic MRCP).
However, although this technique is currently considered to be the gold standard of MRCP, there are some drawbacks associated with it. The larger slice thickness of thick-slab SS-FSE sequences that are larger than the overlying structures can decrease the overall image quality. Detailed diagnostic analysis of the of the biliary system may be adversely affected by projection effects of overlying structures with high T2-weighted signal intensities, such as ascites (Fig. 1.6) or other pathological fluid collections that occur in exudative pancreatitis, pancreatic rupture or postoperative exudates. The diagnostic value of the thick-slab SS-FSE technique is significantly limited in such cases. The overlap between segments of the pancreatic duct, or with cystic lesions, may be a source of problems. Also small intraductal plugs may be missed on these projections. This can be overcome by adapting the section thickness by changing the orientation and positioning of the thick slab to the patient’s duct anatomy, which requires on-site tailoring by the radiologist during image acquisition. The visualization of intraductal content such as stones, protein plugs and hemorrhage may be suboptimal if they are not surrounded by fluid and no signal from solid organs is displayed.
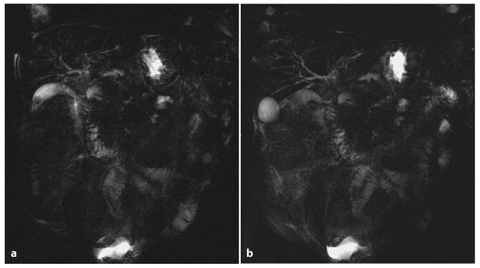
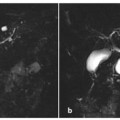
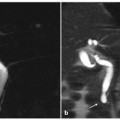
Fig. 1.6
a, b Ascites. Single-slice fast-spin-echo (SS-FSE) magnetic resonance cholangiopancreatography in different orientations show the presence of ascites
1.3.3 Three-Dimensional Turbo-Spin- Echo (3D-TSE) Sequence
The T2-weighted 3D-TSE sequence has been proposed for the purpose of MRCP imaging and may be performed in addition to conventional SS-FSE MRCP images in order to resolve diagnostic doubts and delineate pathologies or variants of the biliary tree [14, 15].
In 3D imaging, one single volume is acquired with contiguous sections and no intersection gaps. An additional phase-encoding gradient along the slice-selection z-axis is required for 3D imaging, in addition to the frequency-encoding and phase-encoding gradients in the x–y plane. The spatial resolution of 3D-TSE sequences is significantly higher in the z




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
