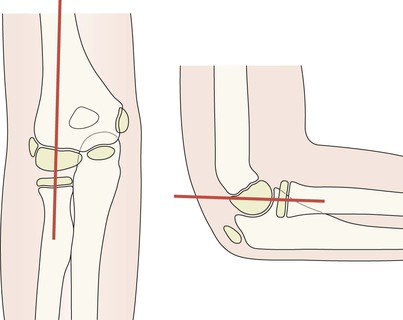
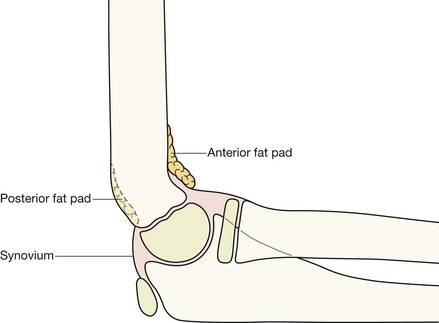
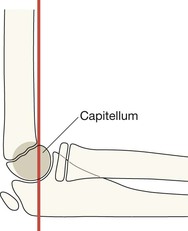
There are pads of fat close to the distal humerus, anteriorly and posteriorly. They are extrasynovial but intracapsular. ▪ Look for the fat pads on the lateral. They are not seen on the AP view. ▪ The fat is visualised as a dark streak amongst the surrounding grey soft tissues. At birth the ends of the radius, ulna and humerus are lumps of cartilage, and not visible on a radiograph. The large, seemingly empty, cartilage filled gap between the distal humerus and the radius and the ulna is normal. From 6 months to 12 years the cartilaginous secondary centres begin to ossify. There are six ossification centres. Four belong to the humerus, one to the radius, and one to the ulna. Gradually the humeral centres ossify, enlarge, and coalesce. Eventually each of the fully ossified epiphyses fuses to the shaft of its particular bone. Exceptions are an occasional normal variant3,4. A 2011 survey4 of 500 paediatric elbow radiographs found: ▪ CRITOL is a really helpful tool when analysing a child’s injured elbow. ▪ Occasionally a minor variation in the sequence may occur. ▪ Use the rule: “I always appears before T”. So, if you see the ossified T before the I then the internal epicondyle has almost certainly been avulsed and is lying within the joint… ie it is masquerading as the trochlear ossification centre (see p. 105). Capitellum Radial head Internal (ie medial) epicondyle Trochlea Is the medial epicondyle slightly displaced/avulsed? A common dilemma. ▪ The rule to apply: ▪ A caveat: ▪ Conclusions: Anterior humeral line (on lateral). Normal alignment: when drawn along the anterior cortex of the humerus, in most normal patients at least one third of the ossifying capitellum lies anterior to this line. Be careful: in very young children the ossification within the cartilage of the capitellum might be minimal (ie normal and age related), and so is insufficiently calcified and does not allow application of the above rule. This line helps you to detect a supracondylar fracture with posterior displacement (pp. 106–108).
Paediatric elbow
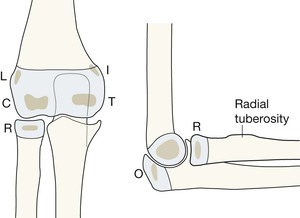
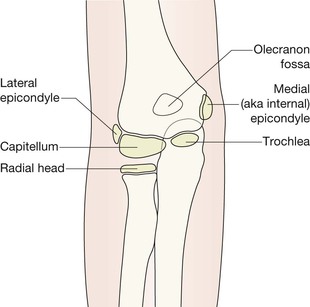
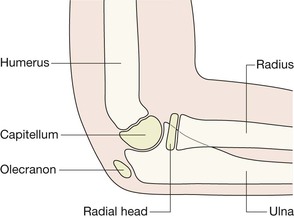
Anatomy
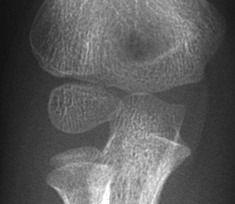
AP view—child age 9 or 10 years
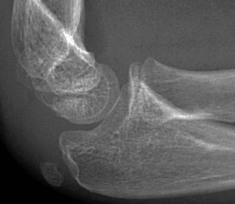
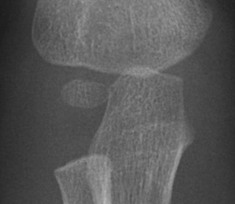
Lateral view—child age 9 or 10 years
Elbow fat pads
AP and lateral: the CRITOL sequence
CRITOL: the sequence in which the ossified centres appear
Exceptions to the CRITOL sequence?
Conclusions


Medial epicondyle—normal anatomy
On the AP radiograph a normally positioned epicondyle will be partly covered by some of the humeral metaphysis.
Occasionally a child in pain will hold the forearm in a position of slight internal rotation. Rotation will project the metaphysis of the humerus away from a normally positioned epicondyle.
When checking the position of the internal epicondyle on the AP radiograph:
AP and lateral—two anatomical lines

Paediatric elbow
7