Fig. 1 a, b.
Supraspinatus outlet. a Diagram shows the supraspinatus outlet (S) bounded by the humeral head (H), the coracoacromial ligament (arrow), acromioclavicular joint and the acromion (a), and the clavicle (c). (Courtesy of Primal Pictures.) b Outlet radio-graph shows the density of the supraspinatus muscle and tendon (s) between the clavicle (c), acromion (a) and humeral head (H)
Clinically, pain can be elicited during abduction and external rotation of the arm or elevation with internal rotation. To provoke a classic Neer impingement sign on physical examination, the examiner raises the patient’s arm forward while simultaneously stabilizing the scapula with another hand, causing the greater tuberosity to impinge against the acromion. If this motion is painful at 90 degrees of forward flexion, it is considered to be positive impingement. The positive result can be confirmed by injection of local anesthetic under the anterior acromion, which will relieve the pain. The Hawkins modification of the Neer maneuver reproduces impingement pain by forced internal rotation at 90 degrees of forward elevation and 30 degrees of forward flexion, which brings the greater tuberosity directly under the coracoacromial ligament, thus simulating the throwing position.
Impingement leads to inflammation of the subacromial bursa and mechanical wear of the tendon. Continued activity can then lead to fibrosis of the subacromial bursa and tendinosis of the supraspinatus tendon. Progression of this condition can lead to partial or full thickness tears of the supraspinatus (Fig. 2). The modified Neer classification system is generally used to describe the stages of impingement as:
Type I: inflammation with no tearing
Type II: partial tear
Type III: full thickness tear
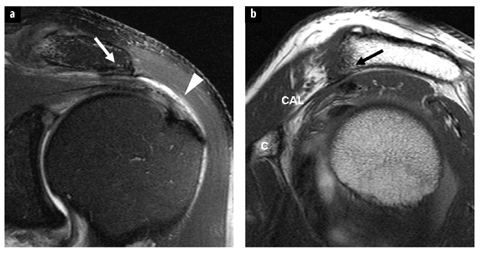
Fig. 2 a,b
Subacromial impingement. Coronal intermediate weighted TSE image with fat-suppression (a) and sagittal T1-weighted TSE (b) images show subacromial spur (arrows) at acromial insertion of coracoacromial ligament (CAL), subacromial/subdeltoid bursitis, and bursal-sided partial tear of supraspinatus tendon (arrowhead). C, coracoid process
Bigliani et al. described three types of acromial morphology (Fig. 3a–c) on outlet radiographs: flat (Type I), curved (Type II) and hooked (Type III), and found the highest incidence of rotator cuff lesions with Type III acromia and the lowest with Type I. However, a hooked morphology as a cause of impingement is controversial since other investigators using both radiographs and magnetic resonance imaging (MRI) have found no association between morphology and cuff tears. Other acromial morphologies that have been described include an inferiorly convex configuration („Type IV”) and a laterally downsloping acromion in the coronal plane (Fig. 3d, e). These shapes are also not agreed upon as causes of impingement. On the other hand, hypertrophic changes at the acromioclavicular joint, whether a result of degeneration or prior trauma, can also narrow the supraspinatus outlet space and cause extrinsic impingement of the supraspinatus tendon.
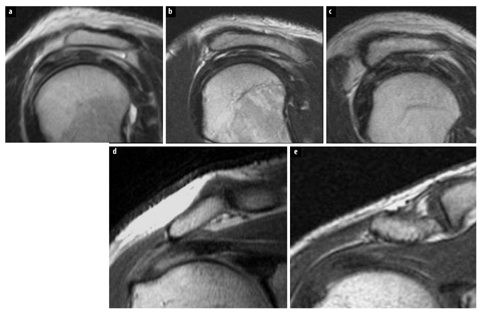
Fig. 3a–e
Acromial morphology. a Flat acromion (sagittal T2-weighted TSE image). b Curved acromion (sagittal T2-weighted TSE image). c Hooked acromion (sagittal T2-weighted TSE image). d Laterally downsloping acromion (coronal T1-weighted SE image). e Inferior convex acromion (coronal T1-weighted SE image)
Subcoracoid Impingement
Subcoracoid impingement refers to compression of the subscapularis tendon, the subcoracoid bursa, and the anterior joint capsule between the coracoid and the lesser tuberosity due to narrowing of the coracohumeral interval (Fig. 4). The narrowing may be congenital due to an elongated coracoid, post-traumatic as a result of deformity of either the coracoid or the humeral head, or iatrogenic such as from a glenoid osteotomy or coracoplasty. Patients typically present with anteromedial shoulder pain and tenderness of the anterior shoulder over the coracoid process. The coracoid impingement test consists of placing the arm in cross-arm adduction, internal rotation and forward flexion to accentuate the pain.
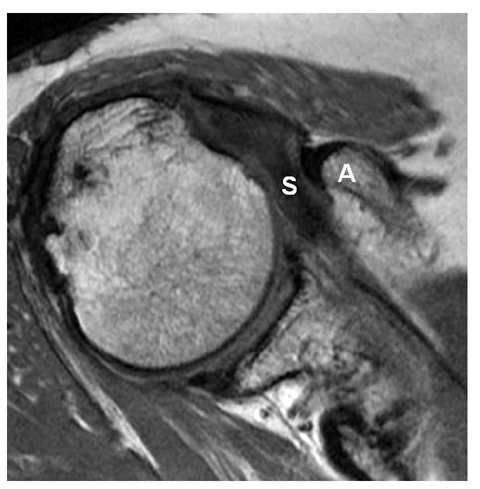
Fig. 4
Subcoracoid impingement. Axial proton density image shows the acromion (A) indenting a tendinotic subscapularis tendon (S)
Attempts have been made to characterize and measure the coracohumeral interval on imaging in order to predict subcoracoid impingement, but there is no consensus. The normal coracohumeral distance has been shown to be 8.4–11 mm, and is on average 1.4–3 mm smaller in females than in males. Subcoracoid stenosis is defined as coracohumeral interval of less than 6 mm, but controversy exists regarding the relationship between coracohumeral distance as determined on magnetic resonance (MR) images and the clinical diagnosis of sub — coracoid impingement. Friedman et al. used cine MRI and shoulder rotation to measure the coracohumeral interval during 10 degree increments from internal to external rotation. Utilizing this technique, they found that, in asymptomatic patients, the normal coracohumeral distance averaged 11 mm in maximum internal rotation, while in symptomatic patients the distance measured 5.5 mm, and there was compression of the subscapularis tendon and other soft tissue structures between the lesser tuberosity and the coracoid process while the shoulder was maximally internally rotated. On the other hand, Giaroli et al., using axial MR images obtained with the humerus in neutral or external rotation, found that none of nine patients in whom subcoracoid impingement was suggested based on the coracohumeral interval measurement alone (average 5.1 mm) had surgical evidence of subcoracoid impingement, whereas a group of seven patients with clinical suspicion of subcoracoid impingement had a coracohumeral distance of 6.2 mm average. Their data showed a poor positive predictive value of MRI, and concluded that subcoracoid impingement could be only supported or suggested by MRI, and not definitively diagnosed.
The arthroscopic definition of subcoracoid impingement is direct contact of the coracoid against the lesser tuberosity. Lo and Burkhart arthroscopically observed the coracoid indenting the subscapularis tendon in patients with subcoracoid impingement and described the tendon rolling over the indentation during internal and external rotation. Based on this „roller-wringer effect” they postulated that indentation of the subscapularis tendon creates tensile forces on the articular surface of tendon, leading to „tensile undersurface fiber failure” (TUFF) of the subscapularis tendon and eventually articular surface tears.
Internal Impingement Syndromes
The internal impingement syndromes involve the articular surface fibers rather than the bursal surface fibers of the rotator cuff, and consist of posterosuperior (glenoid) impingement (classic internal impingement), anterosuperior impingement, anterior impingement and entrapment of the long head of the biceps tendon.
Posterosuperior (glenoid) impingement refers to entrapment of the articular surface fibers of the supraspinatus and infraspinatus tendons between the posterosuperior glenoid labrum and the humeral head. This impingement may occur when the shoulder is placed in the abducted and externally rotated (ABER) position, typically encountered during the late cocking-early acceleration phase of throwing but also experienced in other overhead activities such as tennis and swimming. The „posterior impingement maneuver” on physical examination is positive when posterior shoulder pain is elicited with supine arm abduction of 90–110 degrees and maximal external rotation.
Possible findings on MRI and MR arthrography include: tearing and degeneration of the articular surface of the posterior aspect of the supraspinatus and/or infraspinatus tendons, tear of the posterosuperior glenoid labrum, impaction of the posterosuperior aspect of the humeral head, anterior capsule laxity, and/or posterior capsule thickening (Fig. 5). In baseball pitchers these findings might be associated with a Bennett’s lesion (chronic bone formation at the posterior glenoid rim due to capsular stripping).
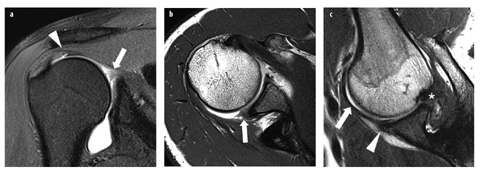
Fig. 5 a–c
Posterosuperior impingement (volleyball player). Coronal T1-weighted magnetic resonance (MR) arthrogram with fat suppression (a) and transverse T1-weigted MR arthrogram (b) show an articular-sided partial tear at the posterior portion of the supraspinatus tendon (arrowhead) as well as degeneration and fraying of the posterosuperior glenoid labrum (arrows). c T1-weighted MR arthrogram obtained in the abduction and external rotation (ABER) position reveals direct contact of the undersurface of the supraspinatus tendon and the posterosuperior labrum (asterisk), degenerative changes of the anteroinferior labrum (arrowhead) and elongation of the IGHL (arrow ). [From: Woertler K (2010)]
Posterior capsular tightening shifts the glenohumeral contact point posterosuperiorly, thus permitting hyper — extension in the ABER position and increased external rotation, with resultant glenohumeral internal rotation deficit (GIRD) and the so-called „dead arm” sensation. These altered glenohumeral mechanics increase the sheer forces and torsional load on the posterosuperior rotator cuff and may also cause rotator cuff undersurface tears. Increased sheering at the biceps anchor and posterosuperior labral attachment can cause superior labrum anteriorposterior (SLAP) IIB lesions.
Anterosuperior impingement refers to entrapment of the articular surface of the superior margin of the subscapularis tendon and the humeral insertion of the biceps pulley (the superior glenohumeral and coracohumeral ligaments) between the humeral head and the anterior superior glenoid rim when the arm is horizontally adducted, maximally internally rotated, and anteriorly elevated to varying degrees. Long head of the biceps tendon abnormalities and undersurface tears of the anterior margin of the supraspinatus tendon may also occur.
Anterior impingement, in which an articular surface tear of the supraspinatus tendon compresses against the anterior superior labrum, clinically mimics the symptoms of classic subacromial impingement, but patients with anterior impingement are usually younger. Arthroscopy may demonstrate: partial articular surface tears of the supraspinatus and subscapularis tendons, SLAP IIA lesions, and internal impingement of the fragmented rotator cuff tissue against the superior labrum just anterior to the biceps anchor during intraoperative performance of the Hawkins test.
Repetitive compression of the long head of the biceps tendon between the humeral head and the glenoid may result in marked hypertrophy of the intra-articular portion of the tendon, having an „hourglass” appearance. The caliber of the hypertrophied intra-articular portion of the long head of the biceps tendon may exceed that of the bicipital groove and thus fail to enter the groove when the arm is elevated. The tendon becomes incarcerated in the joint, and the patient experiences pain and restricted range of motion. Clinically, the patient presents with chronic anterior shoulder pain that is accentuated upon forward elevation of the arm above the head. On physical examination, tenderness is elicited in the region overlying the bicipital groove, and there is loss of the final 10– 20 degrees of passive elevation. Imaging can demonstrate the hypertrophied tendon, and most cases are associated with rupture of the rotator cuff.
Rotator Cuff Disease
Rotator cuff disease is by far the most common cause of shoulder pain and dysfunction in adults. The etiology of this disorder is probably multifactorial with age-related degeneration, metabolic disturbances, impingement, chronic overuse and repetitive microtrauma representing potential contributors. The majority of rotator cuff lesions result from degenerative changes in older individuals with subacromial impingement syndrome. „Traumatic” tears are commonly found with pre-existing degeneration or they might be associated with shoulder dislocation. In athletes, repetitive eccentric stress and intrinsic impingement due to microinstability play a major role in development of rotator cuff tendon lesions at young age.
Tendinopathy
Tendinopathy (tendinosis) represents mucoid tendon degeneration without macroscopic fiber disruption. This process is reflected by increased intrasubstance signal, which is most pronounced on MR images with short echo times. On images with T2 contrast, the signal intensity of the abnormal area is not as high as that of fluid. The affected tendon might become thickened but does not show evidence of fiber discontinuity.
Partial Tears
Partial (partial-thickness) rotator cuff tears can be classified as articular-sided (undersurface), bursal-sided or intratendinous (intrasubstance or interstitial tear). The undersurface of the tendon represents the most common location. With respect to their depth, partial tears can be further characterized with use of the classification system suggested by Ellman:
Grade 1: <3 mm or <1/4 of tendon thickness
Grade 2: 3–6 mm or <1/2 of tendon thickness
Grade 3: >6 mm or >1/2 of tendon thickness
On conventional MRI, fluid-like intratendinous signal intensity on images with T2 contrast represents the diagnostic criterion for diagnosis of a rotator cuff tear. In a partial tear, fluid signal traverses a portion but not the entire thickness of the tendon (Fig. 6). The sensitivity of MRI for the detection of partial rotator cuff tears is limited. It can be increased to over 80% with the use of MR arthrography by improving the detection of articularsided lesions.
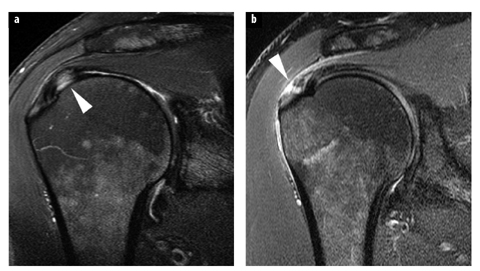
Fig. 6 a, b
Partial-thickness rotator cuff tears. Coronal intermediate-weighted TSE images with fat-suppression show articular-sided (a) and bursal-sided (b) partial tears (arrowheads) of supraspinatus tendon. Note articular cartilage defect of humeral head in b
In recent years some specific types of partial rotator cuff lesions have been described. A delamination tear is typically an articular-sided partial tear in combination with a horizontal intrasubstance tear (horizontal component), which separates the articular and bursal tendon fibers and might lead to medial retraction of the torn articular fibers. This type of tear most commonly occurs in the supraspinatus tendon and has also been described as the PAINT (Partial Articular-sided tear with INTratedinous extension) lesion. In contrast, noncommunicating intratendinous tears have been termed concealed interstitial delaminations (CID). Due to an intact undersurface of the involved tendon, these partial tears might be invisible at arthroscopy and therefore are important to be depicted at imaging.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


