 Clinical Presentation
Clinical Presentation
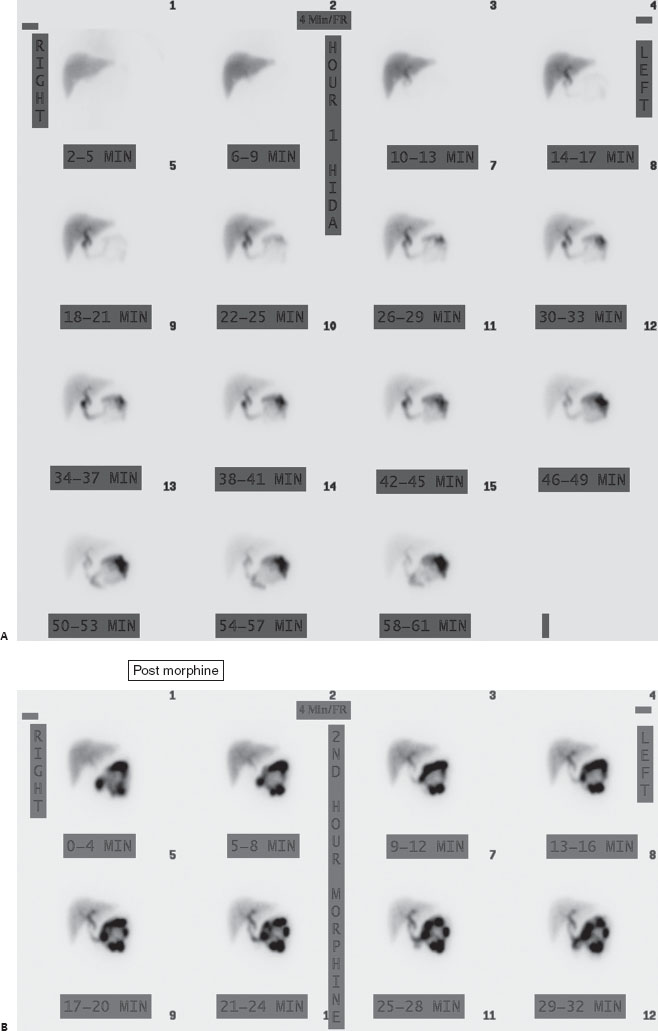
A 40-year-old woman with acute right upper quadrant pain.


HIDA scan sequential imaging over 60 minutes (A in Clinical Presentation) demonstrates excretion of tracer into the duodenum (arrow) but no gallbladder (GB) filling (expected GB location circled). An additional 32 minutes of imaging after morphine administration (B in Clinical Presentation) again fails to demonstrate GB filling.
 Differential Diagnosis
Differential Diagnosis
• Acute cholecystitis: Lack of GB filling, even after morphine administration, is highly suggestive of acute calculous cholecystitis.
• Acalculous cholecystitis: This most often appears identical to calculous cholecystitis on HIDA (no GB filling even after morphine). However, these are typically critically ill inpatients (e.g., with burns, sepsis, or diabetes).
• Chronic cholecystitis: This is usually normal on HIDA scans but may occasionally lack GB filling initially; however, filling will be achieved after morphine or delayed imaging.
 Essential Facts
Essential Facts
• Acute calculous cholecystitis is caused by a stone impacted in the GB neck or cystic duct, leading to venous and lymphatic congestion, GB mucosal edema, inflammation, necrosis, and eventually perforation.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


