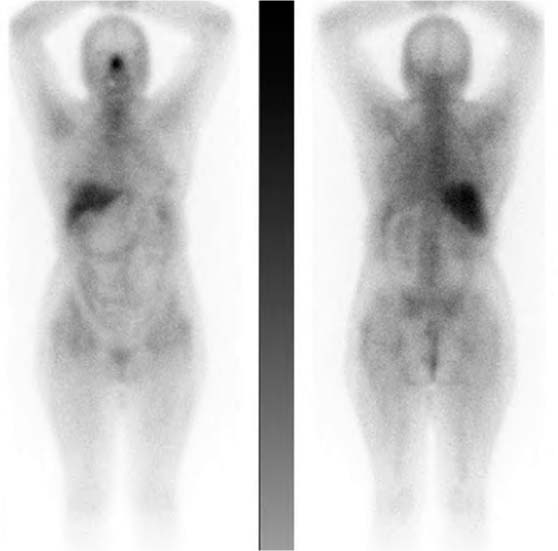
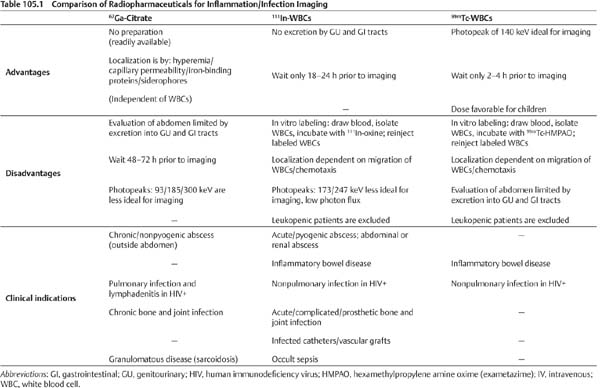
CASE 105 A 68-year-old woman presents with fever of unknown origin. Because of limited venous access, 67Ga is selected as the radiopharmaceutical of choice for evaluation. Fig. 105.1 Whole-body image, anterior, and posterior projections, 67Ga. • A 7.5 mCi dose of 67Ga-citrate is injected intravenously 3 days before scan. • Whole-body imaging in anterior and posterior projections Whole-body images (Fig. 105.1) demonstrate a normal biodistribution pattern. Typically, 67Ga localizes in the nose, salivary glands, lacrimal glands, breasts, liver, spleen, genitalia, and skeleton; it is not unusual to have varying degrees of large-bowel activity. No abnormal tracer localization is seen to suggest active inflammation/infection. • Normal 67Ga scan Normal. No active inflammation/infection identified. Diagnosis final, no clinical follow-up. The best-known and most widely used inflammation/infection–seeking radiopharmaceuticals are 67Ga and autologous white blood cells (WBCs) radioactively labeled with either 111In or 99mTc. Each agent has its advantages, disadvantages, and preferred clinical indications (Table 105.1). As a general principle, they have comparable sensitivity rates on the order of 90% for inflammation, but WBCs are generally more specific than 67
Clinical Presentation
Technique
 Dual-detector gamma camera
Dual-detector gamma camera
 Medium-energy collimators
Medium-energy collimators
 Energy peak at 93-, 185-, and 300-keV photopeaks
Energy peak at 93-, 185-, and 300-keV photopeaks
Image Interpretation
Differential Diagnosis
Diagnosis and Clinical Follow-Up
Discussion
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


