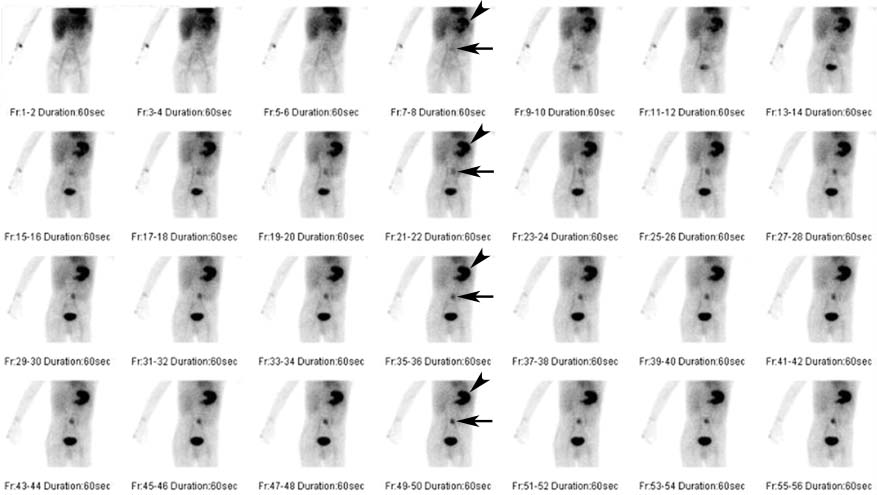
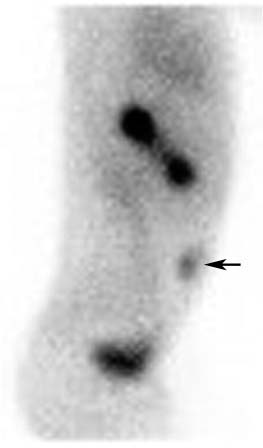
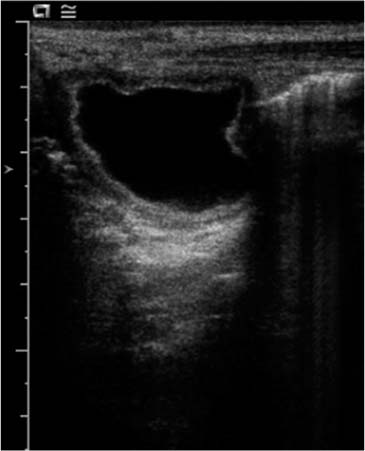
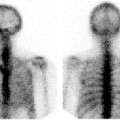
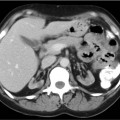
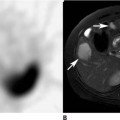
CASE 154 A 5-year-old boy presents with blood in his stool, as well as abdominal pain and constipation. Results of endoscopy of the upper and lower gastrointestinal tract are normal. A Nuclear Medicine study was requested (Figs. 154.1, 154.2, and 154.3). Fig. 154.1 Fig. 154.2 Fig. 154.3 • 99mTc-pertechnetate • Nothing by mouth for 4 to 12 hours. • No barium or Gastrografin for 2 to 3 days before the study. If there is uncertainty as to whether residual oral contrast may interfere with the scan, obtain a radiograph of the abdomen. • Pharmacologic intervention with pentagastrin, histamine H2-receptor blockers, or glucagon has been advocated. These are further discussed in Case 156. • 10 mCi • Intravenous injection • Low-energy, all-purpose collimator • 140-keV photopeak, 20% window • Dynamic imaging of the abdomen and pelvis • Post-void view The flow images (not shown) were normal. The 1-minute images acquired over the ensuing 30 minutes (Fig. 154.1) demonstrate a focus of abnormal accumulation of 99mTc-pertechnetate in the lower abdomen, immediately to the left of midline (arrows). The intensity of uptake in this lesion increases over time in parallel with the normal accumulation within the stomach (arrowheads). There is normal physiologic excretion into the bladder. A single lateral view (Fig. 154.2) confirms the location of the abnormality just deep to the anterior abdominal wall (arrow). A subsequent ultrasound examination (Fig. 154.3) reveals a corresponding fluid-filled structure closely related to the umbilicus, with a “gut signature” wall (alternating hyperechoic and hypoechoic layers).
Clinical Presentation
Technique
 1 frame per second for 60 seconds
1 frame per second for 60 seconds
 1 frame per minute for 30 minutes
1 frame per minute for 30 minutes
Image Interpretation
Differential Diagnosis
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


