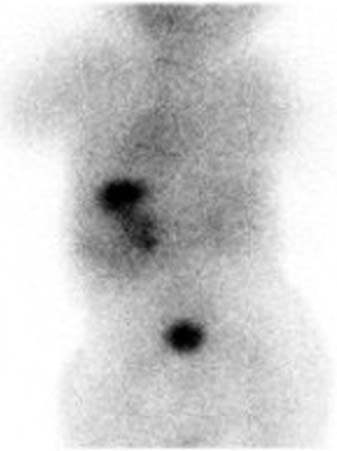
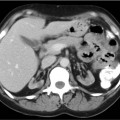
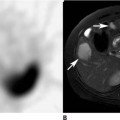
CASE 155 A 7-year-old boy presents with two episodes of blood in his stool. A Nuclear Medicine study was requested (Figs. 155.1 and 155.2). Fig. 155.1 • 99mTc-pertechnetate • Nothing by mouth for 4 to 12 hours. • No barium or Gastrografin for 2 to 3 days before the study. If there is uncertainty as to whether residual oral contrast may interfere with the scan, obtain a radiograph of the abdomen. • Pharmacologic intervention with pentagastrin, histamine H2-receptor blockers, or glucagon has been advocated (see below). • 10 mCi • Intravenous injection • Low energy, all purpose collimator • 140-keV photopeak, 20% window • Dynamic imaging of the abdomen and pelvis • Post-void view, as a Meckel diverticulum may be located adjacent to the bladder Fig. 155.2 The flow study (not shown) was normal. The ensuing 30-minute study (Fig. 155.1) demonstrates normal accumulation within the stomach (arrowheads) and excretion into the bladder. There is also accumulation throughout the study within a structure in the upper abdomen to the left of midline (arrows). A posterior image (Fig. 155.2) reveals this activity to be within the left renal collecting system. • Meckel diverticulum • Enteric duplication or duplication cyst • Hydronephrosis • Regional enteritis • Vascular mass Hydronephrosis. No Meckel diverticulum. The accumulation of 99mTc-pertechnetate in the upper abdomen was within the renal collecting system.
Clinical Presentation
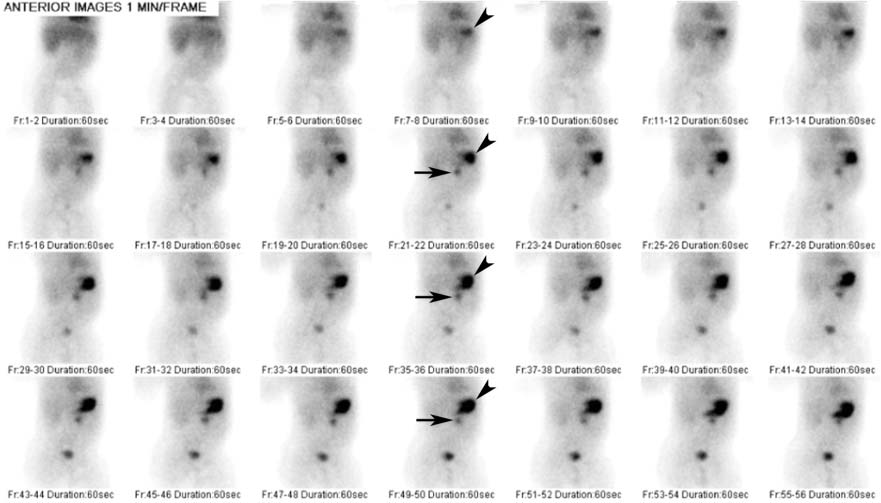
Technique
 1 frame per second for 60 seconds
1 frame per second for 60 seconds
 1 frame per minute for 30 minutes
1 frame per minute for 30 minutes
Image Interpretation
Differential Diagnosis
Diagnosis and Clinical Follow-Up
Discussion
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


