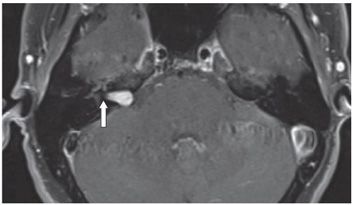
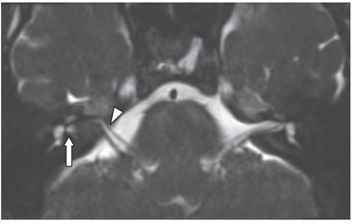
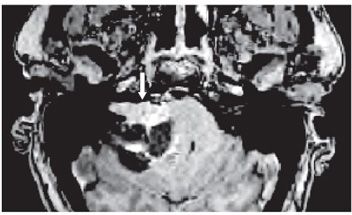
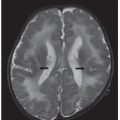
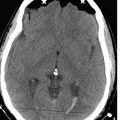
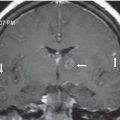
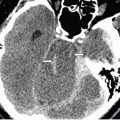
FINDINGS Figure 20-1. NCCT temporal bone. There is a smoothly marginated expansion of the right porus acusticus and internal auditory canal (IAC) as compared with the normal canal on the left side. Note the blunting of the posterior lip (arrow). Figure 20-2. Axial post-contrast volumetric T1 gradient sequence. There is an avidly enhancing lesion filling the majority of the IAC, laterally sparing the fundus with demonstration of a small cerebrospinal fluid (CSF) “fundal cap” (arrow). There is no suggestion of intralabyrinthine tumor extension. Medially, the mass protrudes slightly into the cerebellopontine angle (CPA) cistern. Figure 20-3. Axial T2 cisternographic sequence shows that the tumor arises from the more posterior, vestibular nerve at the level of the IAC, displacing the cranial nerve (CN) VII/VIII complex (arrowhead) anteriorly within the canal. Figure 20-4. Companion case: axial post-contrast T1WI. There is mixed solid and cystic vestibular schwannoma (VS) with the predominately solid, enhancing component within the IAC extending into the anterior aspect of the CPA cistern (arrow).
DIFFERENTIAL DIAGNOSIS VS, CPA and/or intracanalicular meningioma, facial nerve schwannoma.
DIAGNOSIS Vestibular schwannoma (VS).
DISCUSSION NCCT best demonstrates the bony changes of VS. MRI is the examination of choice for evaluation of the total geography of the lesion. T2WI demonstrates replacement of the normal hyperintense CSF signal within the IAC by VS (Figure 20-3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


