The Basilar Artery Trunk
20.1 Case Description
20.1.1 Clinical Presentation
A 39-year-old man collapsed at work and was brought to the emergency department. CT demonstrated a diffuse subarachnoid hemorrhage and associated hydrocephalus. CTA demonstrated an aneurysm at the proximal portion of the basilar artery just distal to its origin from the vertebral arteries. For further evaluation and treatment, the patient underwent conventional angiography.
20.1.2 Radiologic Studies
See ▶ Fig. 20.1.
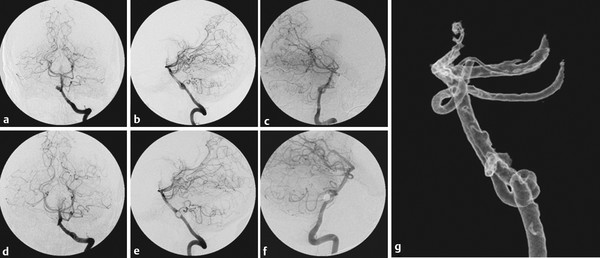
Fig. 20.1 Left vertebral artery (VA) angiogram in anteroposterior (AP) (a,d), lateral (b,e), and oblique (c,f) views with 3D reconstruction (g) before (a,b,c,g) and after (d,e,f) embolization of a saccular basilar trunk aneurysm. 3D rotational angiography revealed its origin to be at the caudal portion of a focal unfused (“fenestrated”) basilar artery pointing cranially. Unassisted coil embolization was performed and resulted in complete obliteration of the aneurysm.
20.1.3 Diagnosis
Ruptured mid-basilar aneurysm in the setting of a proximal focal unfused segment of the basilar artery.
20.2 Embryology and Anatomy
The basilar artery is a result of two simultaneous fusion phenomena that concur with the regression of the primitive trigeminal arteries. When the embryo is about 4 mm long, the primitive posterior circulation is constituted caudally by the paired ventral longitudinal neural arteries that are connected laterally at multiple locations with the primitive hindbrain plexus, and cranially by the caudal divisions of the internal carotid arteries. Cranially, at the pontomesencephalic sulcus, these caudal divisions of the internal carotid arteries fuse to form the basilar tip, whereas caudally, the paired longitudinal neural arteries fuse to form a single basilar artery. The fusion process is typically completed when the embryo is 9 mm long (i.e., around the fifth fetal week). Failure of fusion of the neural arteries and regression of the bridging vessels between longitudinal arteries will lead to varying degrees of nonfusion, from duplicated basilar arteries (as the extreme form of an incomplete fusion process) to focal nonfused segments. The lateral walls of the unfused artery have a normal intrinsic architecture; however, at the base of the medial wall, the media layer is absent. In addition, there is discontinuity of elastin, the subendothelium is thinned, and the muscular layer of the basilar artery can be absent. This structural weakness may lead to the formation of aneurysms at nonfused segments, as the wall architecture resembles those of arterial bifurcations. In addition, one may presume that an incomplete fusion points to an incomplete maturation process of the arterial wall. The lack of cell selection that such pattern, imply may preserve “weaker” (i.e., less matured) endothelial cells, which will later reveal arterial aneurysms when secondary, revealing, triggers, such as hemodynamic stress, are present.
20.3 Clinical Impact
Given the location at the midline, anterior to the brainstem, aneurysms that are associated with a focal unfused basilar artery are best treated with coil embolization.
Because of their embryological development, both limbs of the unfused basilar artery carry brainstem-perforating arteries to their respective sides. Vessel sacrifice of one limb of the fenestration may therefore result in unilateral brain stem stroke resulting from occlusion of perforators and should not be performed.
Failure to recognize a small nonfusion may lead to catastrophic events if the balloon remodeling technique is performed and the balloon is overinflated, which may lead to rupture at the level of the nonfusion site.
20.4 Additional Information and Cases
Four differential diagnoses of a “double lumen of a single artery” have to be discussed that are often mistakenly grouped together under the name “fenestration.”
Given the above-mentioned embryology, a lack of fusion of embryologically paired vessels leads to segmentally unfused arteries. This condition can only exist where two embryological arteries fuse during development; therefore, the basilar artery, as described here, or the anterior spinal artery can harbor unfused segments.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


