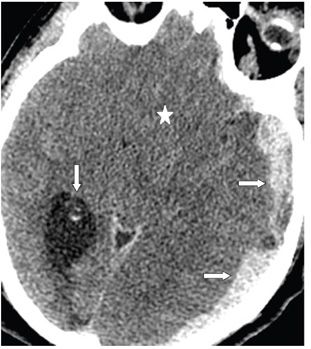

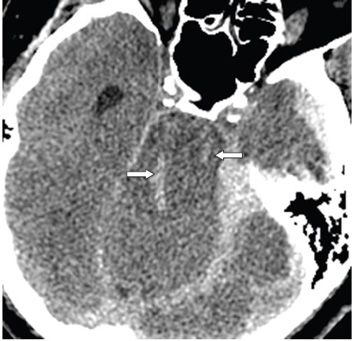
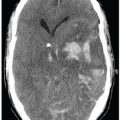
FINDINGS Figure 207-1. Axial NCCT through the tentorial incisura. The upper pons/midbrain (star) is deformed, slightly hypodense, and displaced to the right compressed against the right tentorium (Kernohan notch [KN]). There is effacement of the surrounding interpeduncular, prepontine, perimesencephalic, and quadrigeminal cisterns. The tentorium is dense due to hemorrhage (transverse arrows). There is medial displacement of the left uncus behind the dorsum sella consistent with uncal herniation (UH) (black vertical arrow). The right temporal horn is dilated and trapped (chevron). The cause of the herniation is a large left hyperacute subdural hematoma (SDH) (left lateral transverse arrow). Figure 207-2. Axial NCCT through the suprasellar cistern. There is complete effacement of the suprasellar and interpeduncular cisterns (star), perimesencephalic cisterns, and the quadrigeminal cistern by descending brain tissue transtentorial herniation (central herniation). Structures at the base of the brain such as cerebral peduncles, hypothalamus, chiasm, and the uncus cannot be differentiated. The right trigone (vertical arrow) is dilated. The left hemispheric SDH (transverse arrows) is larger. Figure 207-3. Coronal reformatted NCCT through the tentorial incisura. The tentorium is demonstrated by the vertical arrows. There is effacement of the cerebrospinal fluid (CSF) space around the tentorial incisura due to descent of supratentorial structures (star). There are multiple hyperdense foci in the brainstem (line arrow). These are the Duret hemorrhages (DHs). The third ventricle is effaced and displaced to the right. There is midline shift subfalcine herniation (SFH) from left to right (transverse arrows) by the left hemispheric SDH (chevron). Figure 207-4



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


