28 Trauma
28.1 Spinal Trauma
Traumatic injuries to the spine, either alone or in conjunction with other injuries, are common reasons for visits to the emergency department. Not all injuries to the spine require imaging, and different imaging modalities and workups for spinal injuries are required, depending on the mechanism of injury and symptoms. At times, a high-impact injury may warrant imaging despite the absence of clinical symptoms (e.g., computed tomographic imaging for a patient ejected from a vehicle traveling at 80 mph), and at times neurologic symptoms may warrant further evaluation despite normal findings in other studies (e.g., numbness of an extremity after a motor-vehicle accident [MVA], with normal findings on a computed tomographic study being followed by magnetic resonance imaging [MRI]). Other injuries, which may interfere with the clinical exam, can make it difficult to clinically “clear” a spine as being free of injury. Special considerations exist with children, including the continued role of radiography for evaluation of spinal trauma, in contrast to the situation with adults, for whom computed tomography (CT) has supplanted radiography, and concern about radiation dose, the possibility of mistaking developmental findings for fractures, and the possible need for sedation with MRI (Table 28-1). In the case of the cervical spine, ligamentous injuries are more common in children than in adults, and tend to occur in the upper cervical region, especially in children younger than 8 years of age, as opposed to adults, who more often have injuries of the lower cervical region. Approximately 60% to 80% of spinal injuries in children involve the cervical spine, in contrast to 30 to 40% of spinal injuries involving the cervical spine in adults.
Radiography | Typically, only anteroposterior and lateral radiographs of the spine section being evaluated are needed. Open-mouth odontoid views are not needed in radiography of the cervical spine in children under the age of 8 years. Oblique radiographs and coned-down lumbosacral views are rarely indicated in children. |
Computed tomography | Helical acquisition, three plane bone-algorithm images (less than 3 mm and ideally 1–2 mm slice thickness); axial and sagittal soft tissue algorithm images. |
Magnetic resonance imaging | Include sagittal short tau inversion recovery to investigate for marrow and soft tissue edema. Axial images should be contiguous and parallel (unlike many protocols for adult degenerative disease, which call only for images parallel to the disk space with skip sections). |
Nuclear medicine bone scan | Frontal and lateral projections in whole-body scans. Narrow field-of-view evaluation and possible single-photon emission computed tomography of areas of uncertainty. |
28.2 Anatomic Considerations
In addition to ligamentous laxity, anatomic considerations in interpreting images of the spine in pediatric trauma include the differences in vertebral shape from that in adults and incomplete ossification. In pediatric patients, the stage of ossification varies at different ages, which creates particular uncertainty in the case of C1 and C2 (Fig. 24.2, Fig. 24.3, Fig. 24.4, Fig. 24.5). The alignment of the spine is also different in children, particularly in the cervical spine, which can have a mild kyphosis in young children, as well as “pseudosubluxation” of C1 with respect to C2 (Fig. 24.6).
28.3 Imaging Modalities
28.3.1 Choice of Imaging: Plain Film, Computed Tomography, or Magnetic Resonance Imaging
Plain films and computed tomographic scans are the primary means of detecting fractures and abnormalities of alignment of the spine after traumatic injury. The optimal choice between these imaging modalities is a balance based on the mechanism of injury, symptoms, and concerns about radiation. It is important to keep in mind that although computed tomography (CT) involves greater radiation exposure than does plain radiography, missing a fracture is not an appropriate tradeoff for a lower radiation dose.
Many traumatic injuries warrant CT of the chest, abdomen, and pelvis for evaluating the state of visceral organs. With image acquisition through helical multidetector CT scanners, the thoracic and lumbar spine can be examined via the thin-section bone algorithm reformatting of source data without additional radiation exposure. This therefore constitutes a situation (assuming that CT was already being performed for other reasons) in which plain radiography would expose the patient to greater radiation than would CT. Perhaps the best way to reduce radiation exposure of the pediatric trauma patient is to avoid any imaging when there are no relevant indications for it. Research has shown that clinical examination can be effective in excluding cervical spine injuries, 1 ,? 2 even in children younger than 3 years of age. 3 The development and adoption of criteria for appropriateness of the use of imaging, and additional research on this, will be required, with specific attention to different age subgroups. 4, 5, 6
Magnetic resonance imaging is ideal for evaluating ligamentous injury and seeking signs of cord compression or contusion. However, MRI of the spine may require 20 to 30 minutes per section of the spine, requiring a patient to be away from the patient’s care unit or intensive care unit (ICU) for an extended period, and MRI may require sedation. Although fractures typically show signs of marrow edema on MRI, MRI should not be used as the primary means of detecting a possible fracture. Research has examined the role of diffusion tensor imaging (DTI) for evaluating the integrity of the spinal cord and possibly identifying subtle contusions of the cord, but its use is not yet routine in clinical practice. Magnetic resonance imaging is typically an adjunctive technique, providing additional information in conjunction with CT and other imaging modalities.
Ultrasonography and nuclear medicine imaging are not commonly used in the setting of trauma. Ultrasonography can be used for evaluating a paraspinal hematoma, and radionuclide bone scans can be used for identifying or ruling out suspected compression fractures or acute defects of the pars interarticularis, particularly when there are contraindications to MRI. A nuclear medicine bone scan is sometimes used to investigate suspected abusive trauma.
Determining the appropriate diagnostic workup for a particular pediatric patient, including clinical examination, observation, and imaging, requires multidisciplinary input involving members of the radiology, neurosurgery, orthopaedic surgery, trauma, and pediatric emergency medicine staff.
28.4 Fractures
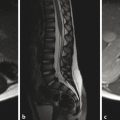
Traumatic fractures of the spine can result from hyperflexion, distraction, or compressive forces. Perhaps the most common type of fracture is a compression fracture. A compression fracture typically involves loss of height resulting from an irregularity in the vertebral superior endplate. If such a fracture is detected on radiographs, CT and MRI are typically performed. Computed tomography is done to fully characterize the fracture, and MRI is done to evaluate for ligamentous and cord injury. When a compression fracture is identified, the degree of height loss should be reported, as should any abnormality in spinal alignment, such as a focal kyphosis. Also important is whether there is retropulsion of the posterior cortex of the vertebral body into the central canal, and if so, a description of the degree of narrowing of the central canal and the effect of the vertebral retropulsion on the spinal cord. Sagittal short tau inversion recovery (STIR) imaging is highly sensitive to marrow edema, and in cases of traumatic injury of the spine typically identifies several adjacent levels of osseous injury. In the setting of trauma, marrow edema without loss of height is considered to represent a bone contusion, probably in the form of trabecular microfractures without cortical disruption (Fig. 28.1).

Vertebral contusions will typically heal completely without loss of height if treated conservatively, particularly through the short-term avoidance of excessive weight-bearing and contact sports. They can, however, predispose to a delayed loss of height if the patient experiences a second traumatic event within a short period after the initial contusive event. For this reason, vertebral contusions may affect the time at which a patient can return to athletic activity.
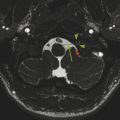
In addition to their susceptibility to traditional osseous fractures, young children with incompletely ossified vertebrae are susceptible to synchondrosis fractures, which are the equivalent of Salter–Harris type I fractures. A particular site of proneness to synchondrosis fracture is the odontoid synchondrosis (Fig. 28.2).

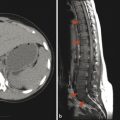
Fractures in adolescents with maturely ossified vertebrae tend to have features and patterns on imaging that resemble those in young adults. A three-column hyperflexion-distraction injury of the spine, known as a Chance fracture (Fig. 28.3), is an unstable fracture that must be rapidly identified. This pattern of injury is most commonly seen when passengers in a car are restrained with a lap-belt alone, and its incidence has decreased in the era of child seats and three-point seatbelts.

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


