 Clinical Presentation
Clinical Presentation
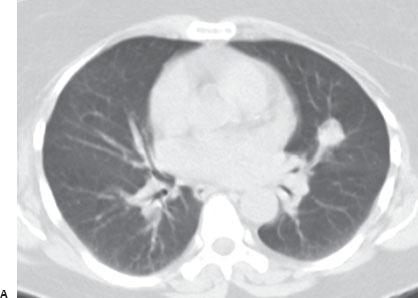
A 53-year-old woman presents with a newly diagnosed solitary pulmonary nodule.
Further Work-up
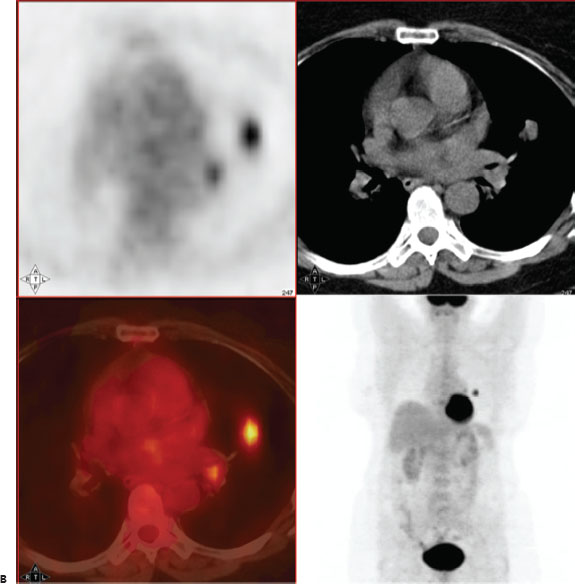

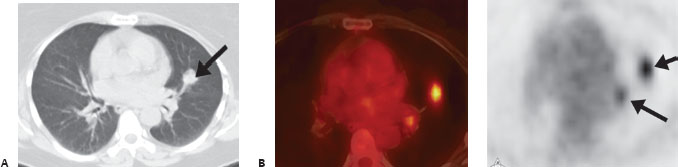
(A) Chest CT demonstrates a 1.5-cm noncalcified nodule in the left upper lobe (arrow). (B) FDG-PET/CT and PET demonstrate markedly increased activity to both the left lung nodule and a left hilar lymph node (arrows).
 Differential Diagnosis
Differential Diagnosis
• Lung cancer with ipsilateral hilar metastasis: A hypermetabolic solitary pulmonary nodule (SPN) is lung cancer until proven otherwise; ipsilateral hypermetabolic mediastinal lymph nodes usually indicate regional metastases.
• Tuberculosis (TB): Active TB can be markedly hypermetabolic in the parenchyma and hila. However, the parenchymal lesion is often more infiltrative or cavitary; inactive TB may be calcified on CT and have lower FDG uptake.
• Sarcoid:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


