The Meningeal Supply
31.1 Case Description
31.1.1 Clinical Presentation
A 53-year-old woman presented with a history of seizures.
31.1.2 Radiologic Studies
See ▶ Fig. 31.1, ▶ Fig. 31.2.
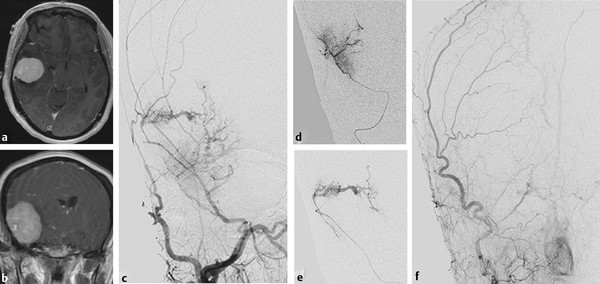
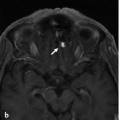
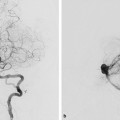
Fig. 31.1 Axial (a) and coronal (b) contrast-enhanced T1-weighted MRIs demonstrate a right frontotemporal densely and homogeneously enhancing convexity meningioma with perifocal edema and midline shift. Neurosurgery requested a preoperative angiography to determine its vascularity with potential embolization if the tumor was deemed hypervascular. Right external carotid artery (ECA) angiogram in anteroposterior view (c) reveals two MMA branches with sunburst-type supply to the tumor. Both branches were subsequently injected (d,e). After polyvinyl alcohol particle embolization, complete devascularization of the tumor can be seen on the control angiogram (f).
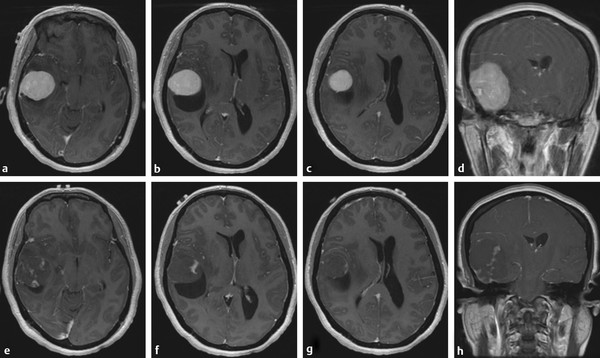
Fig. 31.2 Preoperative (a–d) versus postoperative (e–h) contrast-enhanced T1-weighted MRIs demonstrate the effect of PVA embolization with intratumoral necrosis and significant decrease in contrast material uptake.
31.1.3 Diagnosis
Meningioma fed by two separate branches of the middle meningeal artery (MMA).
31.2 Anatomy
There is considerable variation in the supply to the dura. We limit our description to the “classical” dural arterial anatomy and some of the more common arterial variations. There will be some overlap with other cases regarding the descriptive anatomy of the vessels supplying the dura; however, the major focus of this case is to describe the arteries that are involved in the supply of the dura mater and that, therefore, may play a role both in the embolization of dural arteriovenous fistulas (dAVF) and in the preoperative devascularization of cranial meningiomas. See also Cases 3, 5, 7, 25, 26, 27, 28, and 30.
The MMA arises from the internal maxillary artery and is the most important source of cranial dural supply. It enters the cranium via the foramen spinosum and makes a sharp turn as it enters the middle cranial fossa. It has frontal, temporal squamous, petrous, cavernous-ophthalmic, and parietal branches. Posterior branches course toward the sigmoid sinus and the transverse sinus and contribute medially to the supply of the tentorium. Cranially, the MMA anastomoses at the level of the superior sagittal sinus with the anterior falcine artery.
The accessory meningeal artery arises either from a common trunk with the MMA or distal to the MMA. It courses more medially and anteriorly compared with the MMA, toward the cavernous sinus region, where it anastomoses with the inferolateral trunk (ILT) at the level of the foramen ovale and (despite its name) supplies only a very small portion of the dura in this region.
The neuromeningeal trunk of the ascending pharyngeal artery supplies, via the hypoglossal and the jugular branches, the dura surrounding the respectively named foramina. At the level of the hypoglossal canal, the hypoglossal artery connects to the odontoid arcade, which interconnects to the C3 branches of the vertebral artery system, thus supplying the dura around the foramen magnum and dens. The hypoglossal artery may give rise to the artery of the falx cerebelli and the posterior meningeal artery (see Case 30’s ▶ Fig. 30.5 for an example). Its clival branches supply the inferior clivus and anastomose with the internal carotid artery (ICA). The jugular branch supplies the dura of the jugular foramen and the lateral clivus and may extend cranially toward Dorello’s canal (abducens nerve) and, further laterally, toward the sigmoid sinus, where it can anastomose with the MMA and the transosseous dural branches of the occipital artery.
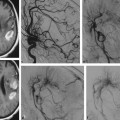
The occipital artery usually supplies the dura of the posterior fossa via a transmastoid branch that runs through the bone into the lateral posterior fossa. Although this transmastoid artery may also arise from the ascending pharyngeal artery and the posterior auricular artery, it is most commonly seen to arise from the distal occipital artery (▶ Fig. 31.3). In rare cases, the occipital artery can give rise to the posterior meningeal artery or the artery of the falx cerebelli. In shunting dural lesions, small osteodural branches will be recruited that traverse through the bone. As they are typically—even in the presence of a shunt—very small and tortuous, it is unlikely that liquid embolic material with a short polymerization time will reach the shunt through these vessels (▶ Fig. 31.4).
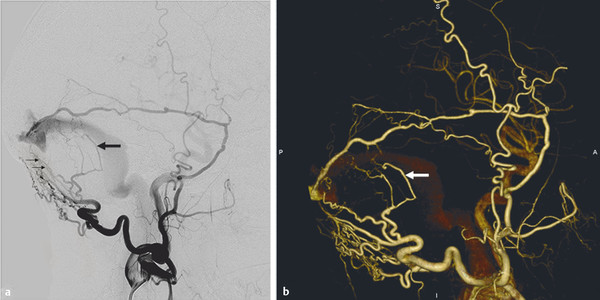
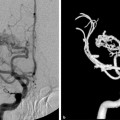
Fig. 31.3 Lateral left ECA angiogram (a) and 3D reconstruction (b) reveal that the occipital artery contributes to the supply of the dura via transmastoidal (the stylomastoid branch, arrow) and transosseous (small arrows) branches that, in this case of a dural shunt, demonstrate anastomoses with the MMA.
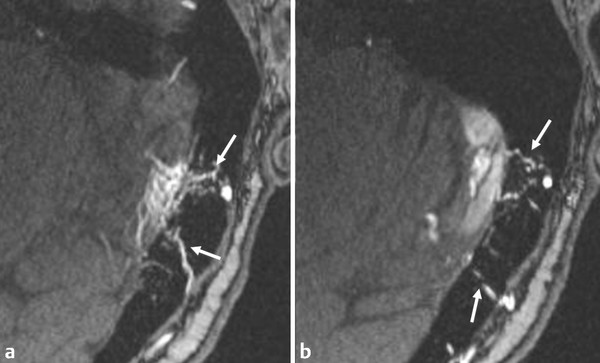
Fig. 31.4 In a patient with a dural arteriovenous fistula of his left transverse sinus, time-of-flight MRA at 3 T (axial source data, a,b) demonstrates the osteodural contribution (arrows) from the occipital artery piercing the bone to contribute to the supply to the fistula. Given the fine network of these osteodural arteries in the supply of dural-based lesions, deep penetration of liquid embolic material is more difficult to achieve through these vessels then through the more direct feeder arising from the meningeal vessels. This is of particular importance when using embolic material that polymerizes quickly, such as glue.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


