4 Basal Ganglia/Dentate Nuclei Mineralization
4.1 Case Presentation
4.1.1 History and Physical Examination
A 62-year-old woman with past medical history of type 2 diabetes mellitus (DM) presents with right lower extremity edema, pain, fever and confusion. The patient was admitted to the emergency room for cellulitis of the right lower extremity and altered mental status.
The patient is febrile. Her cranial nerves II–XII were intact with no focal neurologic deficit.
4.1.2 Imaging Findings and Impression
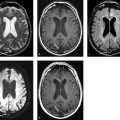
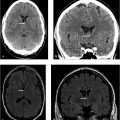
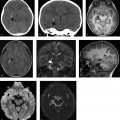
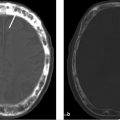
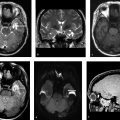
Axial CT scans of the head without contrast (▶ Fig. 4.1a,b) show hyperdensities (HU of 110) involving the bilateral basal ganglia and the bilateral dentate nuclei (black arrows). Axial gradient-echo images (▶ Fig. 4.1c,d) show susceptibility artifact in the corresponding areas consistent with calcification (white arrows). The calcifications are symmetric without associated edema or mass effect.

4.2 Differential Diagnosis
Basal ganglia calcification:
Bilateral calcification involving the basal ganglia with a predominance for globus pallidus interna seen as hyperdensity on CT and presence of susceptibility on gradient-echo images.
Fahr’s syndrome:
Rare genetic disorder of abnormal vascular calcium deposition.
Presents as symmetrical calcifications of the bilateral globus pallidus, caudate, lentiform nucleus, thalamus, and dentate nucleus.
MR images may be normal or have hyperintense signal on the T1-weighted images.
PET scan may show degrees of fluorodeoxyglucose (FDG) uptake.
Should be differentiated from underlying metabolic causes such as hyperparathyroidism and hypoparathyroidism by measuring serum calcium, phosphorus, and alkaline phosphatase levels.
Mineralizing microangiopathy:
Usually seen in children receiving chemotherapy or radiotherapy.
Areas typically involved are the gray–white matter interface, lentiform nucleus, and dentate nucleus of the cerebellum.
Mitochondrial encephalomyopathy, lactic acidemia, and stroke-like symptoms (MELAS):
MELAS is a mitochondrial disease with maternal inheritance.
Presents in younger adults with multiple strokes in different stages of development, not confining to a specific vascular territory.
CNS tuberculosis:
Multiple punctate calcified and noncalcified lesions involving bilateral cerebral hemispheres, including the basal ganglia.
Since the noncalcified lesions are active granulomas, they tend to enhance with gadolinium administration.
Cockayne’s syndrome:
Rare genetic dysmyelinating disorder. Patients are children with neurodevelopmental delay and hearing and skin problems.
On brain MR images, there is atrophy of cerebellum, corpus callosum, brain stem, and supratentorial white matter.
TORCH (toxoplasmosis, other [syphilis, varicella-zoster, parvovirus B19], rubella, cytomegalovirus, and herpes) infection.
Congenital HIV infection and HIV encephalopathy may have basal ganglia calcifications which are NOT seen when the virus infection occurs later in life.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


