 Clinical Presentation
Clinical Presentation
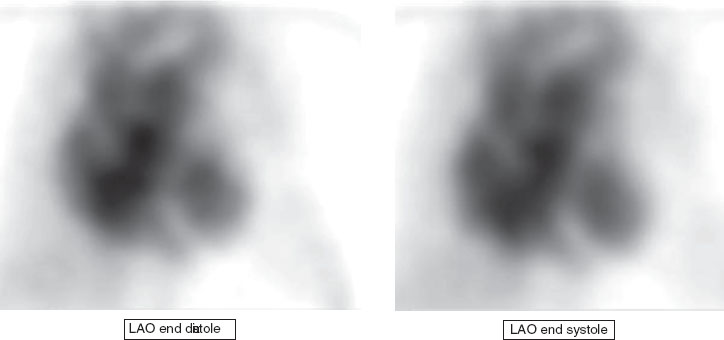
A 64-year-old man with progressive shortness of breath.

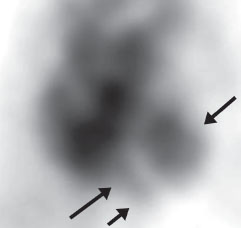
Two left anterior oblique (LAO) frames at end diastole (ED) and end systole (ES) from a Tc99m RBC MUGA scan demonstrate a significantly dilated left ventricle (LV; single arrow) compared with the normal right ventricle (RV; double arrows). Only a slight decrease in LV size is seen on end systole compared with end diastole (left ventricular ejection fraction [LVEF] calculated to be 32%). The visualized portions of the RV demonstrate normal size and wall motion.
 Differential Diagnosis
Differential Diagnosis
Decreased resting LVEF and ventricular dilatation are nonspecific and can be seen with ischemic disease, valvular disease, and cardiac toxicity.
• Ischemic cardiomyopathy: A regional wall motion abnormality is most specific for ischemic disease, although global wall motion abnormalities can also be seen, as in this case. The RV is typically spared, as also in this case.
• Chemotherapy: Certain regimens, such as doxorubicin, are potentially cardiotoxic. Effects are dose-dependent and usually transient. RV and LV dilatation may be seen. Alcohol is another toxin that can cause this same dilated cardiomyopathic appearance.
• Aortic regurgitation:
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


