Introduction
Artifacts are common in nuclear medicine. It is good judgment to think of an artifact or medical device first when there is an unusual finding (Patton, 1994). Nuclear medicine imaging relies on the detection of photons originating within the body from an administered radiopharmaceutical. In this regard, the anterior view of the body will be different than the posterior view, and artifacts may not be evident on all the views from a nuclear medicine study.
Nuclear medicine studies produce physiologic information. They are sometimes very sensitive for detection of disease not easily found by other imaging means. However, normal physiologic alterations in body function – fasting versus non-fasting, exercise versus non-exercise, and so forth – may lead to significant changes in nuclear medicine studies without significant pathologic or morphologic changes in the patient. Because nuclear medicine studies (excluding hybrid scanners with CT or MRI) also have poor anatomic information in comparison with other imaging techniques, artifacts or medical devices that are easily identifiable on other imaging studies may be difficult to identify on nuclear medicine images, particularly for the inexperienced observer. It is always wise to correlate any imaging study, whether it is ultrasound, CT, nuclear medicine, or MRI, with other imaging studies. This is a good habit which reduces errors, improves patient care, and saves more time than it costs to look through the other studies (Patton, 1994).
This discussion concerns artifacts related to medical devices and foreign bodies. Many nuclear medicine artifacts arise from technical aspects of nuclear medicine imaging, such as instrumental settings, radiotracer quality control, and drug effects (Zanzonico, 2008). These artifacts related to technique will not be discussed here because they are covered more extensively in standard nuclear medicine texts and articles (Gentili et al., 1994; Mainor, 2009; Mettler, 2012; Ryo et al., 1990; Zanzonico, 2008).
Normal Adult and Pediatric Anatomy
Normal whole-body pediatric and adult bone scintigraphy with technetium 99m (Tc-99m) methylene diphosphonate (MDP) displays different features (Figure 9.1). In the pediatric population there is intense radiotracer uptake in the growing physes of long bones. Normal adult whole-body planar bone scans with Tc-99m MDP demonstrates normal expected uptake in the bilateral sacroiliac joints, iliac crest, acromioclavicular joints, sternoclavicular joints, and nasal region. Normal radiotracer activity is excreted into the kidneys and urinary bladder.
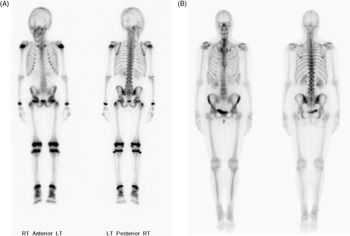
Figure 9.1 (A) Normal pediatric whole-body Technetium 99m-methylene diphosphonate (Tc-99m MDP) bone scan displays intense expected radiotracer uptake in the physes of long bones. (B) Normal adult whole-body bone scan Tc-99m MDP demonstrates normal expected uptake in the bilateral sacroiliac joints, iliac crest, acromioclavicular joints, sternoclavicular joints and nasal region. Normal radiotracer activity is excreted into the kidneys and urinary bladder.
Normal fluorine 18 fluorodeoxyglucose (FDG) PET scanning and fluorine 18 sodium fluoride (NaF) PET bone scans have very different patterns of uptake (Figure 9.2). F18-FDG PET has intense uptake in the brain as well as renal excretion of the isotope. Typically, there is mild activity in the bone marrow of the axial skeleton.
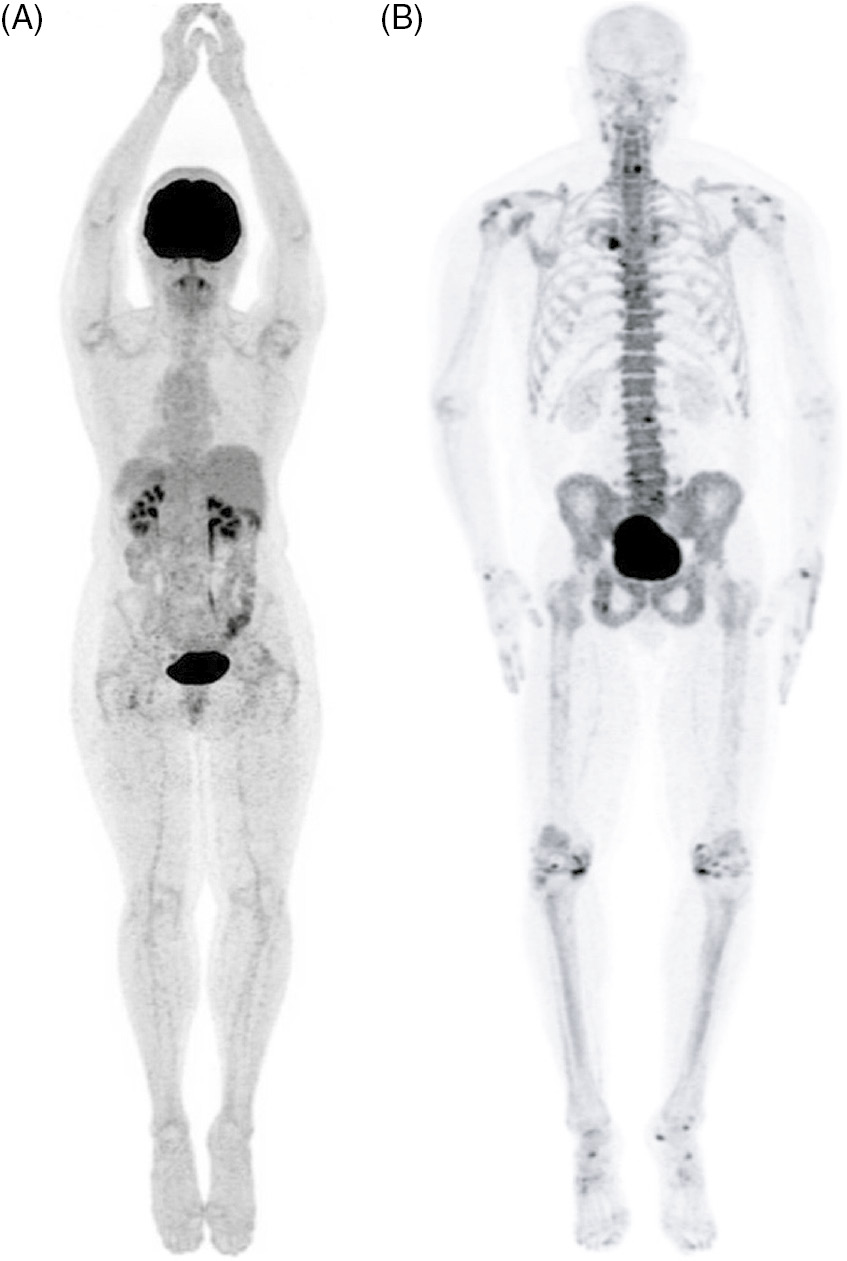
Figure 9.2 (A) Whole-body F18-FDG PET scan maximum intensity projection (MIP) bone demonstrates intense uptake in the brain and renal excretion. Mild activity is seen within the bone marrow. (B) Whole-body F18-NaF PET bone scan MIP demonstrates scattered focal uptake within the spine, bilateral knees, feet and shoulder joints consistent with degenerative bone remodeling. Note: Intense uptake is seen within the brain on FDG PET and no uptake is seen on NaF PET.
While FDG is an analog of glucose, the fluoride in NaF incorporates into the hydroxyapatite (mineral) component of bone by replacing a hydroxyl group to form fluoroapatite. F18-NaF PET bone scan commonly demonstrates non-malignant, scattered focal uptake within the spine, bilateral knees, feet, and shoulder joints, consistent with degenerative bone remodeling. Normally, there is no brain uptake on NaF PET scanning.
Orthopedic Prostheses
Orthopedic devices may produce troublesome, bizarre images if one is not familiar with their effects. They can cause active bone formation with a “positive” bone scan, or they can block photons from decay of radiotracer originating deeper in the body. Many of the devices and surgical constructs – spine struts, knee prostheses, hip prostheses, spinal fixation apparatus, skull plates, and large-fracture fixation plates – have a characteristic appearance. They are readily explained if the patient’s surgical history and radiographic studies are available for comparison (Patton, 1994).
Technetium MDP bone scans often show typical photopenic defects involving knee prostheses in the distal femur and tibial condyles (Figure 9.3). FDG–PET imaging is sometimes performed for evaluation of primary and secondary bone malignancies. Large prostheses, particularly large limb-sparing prostheses, produce streak artifact and photopenia from scatter of the photons from the annihilation of positrons emitted from F-18 (Figure 9.4). Typical prostheses placed for degenerative arthritis or after a hip fracture will show photopenia at the prosthesis site and periprosthetic FDG uptake (Figure 9.5A–D).

Figure 9.3 Tc-99m MDP bone scan shows photopenic defects involving bilateral knee joints in the region of femoral and tibial condyles.

Figure 9.4 (A) 50-year-old women with history of osteosarcoma of left distal femur status post resection and limb-sparing prosthesis. (B) Left to right, top to bottom, axial bone window CT and FDG PET, fused axial and coronal images of the lower thigh demonstrate the prosthesis within the distal left femur producing streak artifact and photopenia on the PET images.

Figure 9.5 60-year-old women with right hip hemiarthoplasty. Axial CT bone window image (A) demonstrates right hip prosthesis. Axial bone window (B) non-attenuation corrected (NAC) and attenuation corrected (AC) FDG PET (C), fused axial and coronal (D, E) images of the pelvis demonstrate the right femoral prosthesis with photopenia in the region of prosthesis. Periprosthetic FDG uptake is seen on AC and fused images and is minimally seen on the NAC image, consistent with attenuation correction artifact.
Sodium fluoride (NaF) PET images may show intense radiotracer uptake in bone surrounding a prosthesis (Figure 9.6). This represents active boney remodeling. This can last for years and is not pathologic. It often most intense in the first six months after surgery (Patton, 1994). Stable uptake consistent with ongoing reparative bone remodeling is also evident on Tc-99m bone scans and should not be confused with malignant recurrence (Figure 9.7A–D). This can last for many years and is not pathologic unless the patient complains of new pain, in which case one should consider loosening, infection, or local recurrence of tumor. In some cases, reparative remodeling is a bony reaction to unusual stress placed on the bone (Figure 9.8A,B). In all cases, it is best to correlate the patient’s nuclear medicine imaging with his or her clinical picture, laboratory results, and other imaging studies.

Figure 9.6 49-year-old women with right hip hemiarthroplasty. Maximum intensity projection images of CT with bone window (A), NaF PET (B), and fused PET-CT image (C) demonstrate right femoral prosthesis with intense NaF uptake in the proximal femur surrounding the prosthesis, representing reparative bone remodeling. This can last for years and is not pathological.

Figure 9.7 15-year-old girl with history of osteosarcoma of left femur status post resection and prosthesis. (A) Lateral and (B) AP radiographs of the left knee show a distal femur limb-sparing prosthesis and knee arthroplasty. Tc99m whole-body bone (C) anterior and (D) posterior projections at different window settings demonstrate mild diffuse increased radiotracer activity around the distal end of the femur prosthesis and proximal end of tibial prosthesis, representing reparative bony remodeling. This can last for many years and is not pathological unless patient complains of new pain, in which case one should consider loosening, infection, or recurrence of tumor.

Figure 9.8 40-year-old man with history of facial trauma, status post mandibular reconstruction. (A) A mandibular radiograph demonstrates mandibular reconstruction on the right side with loss of bone and teeth. (B) Tc-99m MDP bone scan demonstrates uptake within the body of mandible on the left side which is due to altered stress from chewing.
Infection; Hardware Loosening; Reparative Remodeling; Synovitis
Nuclear medicine imaging along with MRI and CT is often a sensitive method for diagnosing osteomyelitis (Figure 9.9). With three-phase bone scans, blood flow and blood pool images show increased radiotracer in the soft tissues around the infected bone and increased radiotracer in the infected bone on delayed imaging. Indium-111 tagged WBC scans give good results for identifying a prosthetic joint infection in the right clinical setting (Figure 9.10). Hardware loosening may be secondary to infection, but it may also occur without an infection being present. Its radiographic appearance can be unremarkable, and its appearance on Tc-99m MDP studies may resemble those seen with a prosthetic infection (Figures 9.11 and 9.12).
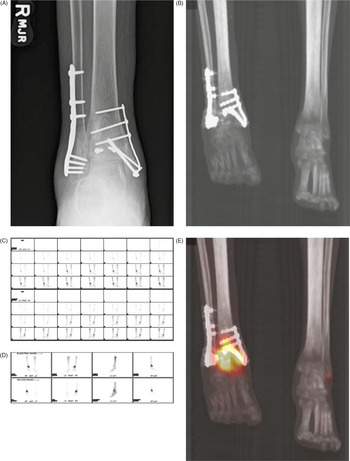
Figure 9.9 30-year-old man with history of bimalleolar right ankle fracture status post fixation (A,B) presented with fever and sepsis. Technetium 99m MDP bone scan shows increased radiotracer around the right ankle on blood flow (C), blood pool (D), and delayed MIP fused images (E) consistent with osteomyelitis.

Figure 9.10 55-year-old man status post total right knee arthroplasty (A) presented with right knee pain and fever. Indium-111 tagged WBC scan planar images show increased localization of radiotracer around the prosthesis (B) consistent with prosthetic joint infection in this clinical setting.

Figure 9.11 65-year-old woman with right knee arthroplasty with persistent knee pain. Increased radiotracer uptake on the blood flow (A), blood pool and delayed images (B), delayed MIP SPECT (C), and fused (D) images around the prosthesis are consistent with hardware loosening (given the patient’s lack of infectious signs and symptoms).

Figure 9.12 50-year-old man with history of partial right medial knee hemiarthroplasty with persistent knee pain. Increased radiotracer uptake on the blood flow (A), blood pool (B), delayed MIP SPECT (C) and fused (D) images in the medial compartment are consistent with hardware loosening (lack of infection symptoms). Focal radiotracer uptake in the lateral right femoral condyle is due to degenerative changes.
The distinction between an infected versus non-infected prosthesis is often made based on the clinical picture. In those patients lacking clinical signs of an infection (fever, redness, localized swelling, elevated WBC count, and so forth) a diagnosis of hardware loosening or a reparative bony remodeling process is made. Frequently, these patients will have to undergo surgery to address the loosening and to ascertain for sure there is no soft tissue or bone infection.
Degenerative disease with osteophyte formation and sclerosis also is a common cause for increased radiotracer uptake (Figure 9.13). Reparative bony remodeling changes may be evident in patients with paraplegia or quadriplegia (Figure 9.14). This in part may be from heterotopic bone formation, and any nuclear medicine studies in these patients should be closely correlated with the patient’s radiographic images and clinical picture (Figure 9.14E).
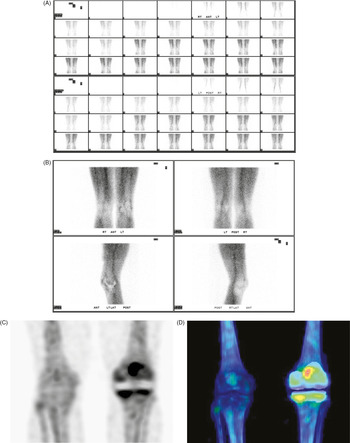
Figure 9.13 54-year-old man with history of right knee arthroplasty presented for chronic knee pain. Technetium 99m MDP bone scan shows no abnormal increased radiotracer activity on (A) blood flow and (B) blood pool images. Multiple foci of radiotracer uptake around the right knee prosthesis on (C) delayed MIP SPECT and (D) fused images are consistent with degenerative/reparative/remodeling changes.

Figure 9.14 24-year-old paraplegic man presented for fever of unknown origin. Technetium 99m MDP bone scan shows no abnormal increased radiotracer activity on (A) blood flow or (B) blood pool images. Multiple foci of radiotracer uptake around the both hip joints on (C) delayed MIP SPECT and (D) fused images are consistent with remodeling changes as seen on (E) MIP bone image. Increased radiotracer activity in the lower lumbar spine is also related to remodeling.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


