The Anterior Choroidal Artery
9.1 Case Description
9.1.1 Clinical Presentation
A 50-year-old woman presented to the emergency department with acute onset of headache. CT demonstrated a subarachnoid hemorrhage, and digital subtraction angiography was performed.
9.1.2 Radiologic Studies
See ▶ Fig. 9.1.
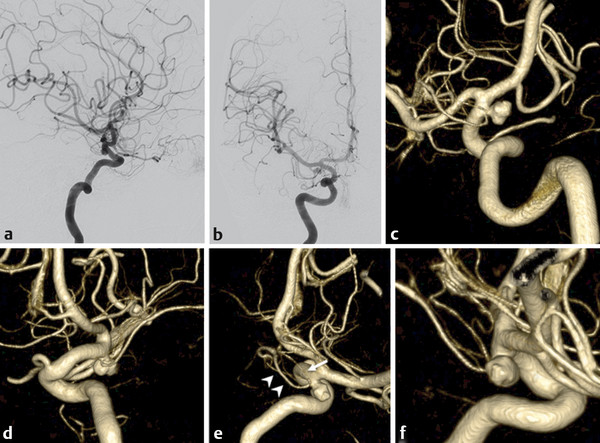
Fig. 9.1 Right ICA angiograms in lateral (a) and anteroposterior (b) views and 3D rotational reconstruction (c–f) demonstrate a 4-mm narrow-necked inferolaterally directed aneurysm that is situated cranial to the origin of the AChoA. The AChoA appears duplicated, with the superior smaller branch (white arrow) having a short medial course toward the uncus and the larger branch (arrowheads) extending to the choroidal fissure.
9.1.3 Diagnosis
Anterior choroidal artery (AChoA) aneurysm in the setting of a duplicated AChoA.
9.2 Embryology and Anatomy
In its developmental anatomy, the internal carotid artery (ICA) ends with a bifurcation into a rostral (cranial) and a caudal branch. In adult life, the rostral branch will give rise to the ICA distal to the posterior communicating artery (PcomA), the AChoA, the anterior cerebral artery (ACA), and the middle cerebral artery. The caudal branch will form the PcomA, parts of the basilar artery, and the posterior cerebral artery (PCA). The cranial division gives rise to a prominent ACA and AChoA at the “choroidal” stage of development (roughly 5 weeks), which supply the choroid plexus and anastomose at the interventricular foramen with each other via their respective choroidal branches. In addition, both vessels also give rise to perforating diencephalic and telencephalic branches that course toward the vesicles (i.e., the later hemispheres), with the AChoA supplying the more posterior aspect of the vesicle.
At this stage, the caudal division gives rise to the posterior choroidal artery that anastomoses with the AChoA at the atrium. As a result of hemispheric growth and increased antegrade flow of the basilar system that connects to the caudal division of the ICA, the telencephalic branches of the posterior choroidal artery will annex the telencephalic territory previously supplied by the AChoA and will form the later PCA. Thereby, the posterior choroidal branch adopts the hemispheric supply from the AChoA. As the hemispheres grow further, the volume of brain supplied by the AChoA diminishes in favor of the PCA. However, many variations in the territories of the ACA, PCA, and the AChoA exist and can be explained by the aforementioned embryological considerations. As the AChoA provides the main blood supply to the posteromedial aspects of the growing cortex during the early stages of development, it is conceivable that when the telencephalic branches of the embryonic posterior choroidal artery fail to take over this territory, cortical branches of the AChoA may persist as the main supply to the temporal, parietal, and occipital lobes. In fact, a spectrum of variations exists, ranging from a single cortical branch originating from the AChoA to complete replacement of the PCA by branches of the AChoA.
The AChoA typically originates distal to the PcomA as the first branch of the cranial division of the embryonic ICA from its posterior wall. Although “duplications” of the AChoA have been reported, they are presumably related to separate origins of the uncal (or telencephalic) branch and the diencephalic or choroidal branch of the AChoA from the ICA.
The typical course of the AChoA can be divided into the cisternal and intraventricular segments. In most instances, the AChoA courses through the perimesencephalic cistern, along the cerebral peduncles, and is in close proximity to the basal vein of Rosenthal and the optic tract. Anterolateral to the lateral geniculate body, the AChoA enters the choroidal fissure to reach the choroidal plexus of the temporal horn. The point of entry into the ventricle has been termed the plexal or choroidal point and is important, as no further brain-supplying vessels are derived from the AChoA beyond this point. It can be identified by the characteristic bend the artery makes (steep downward course for a few millimeters, followed by a sharp posterior turn) when entering the choroidal fissure (▶ Fig. 9.2).
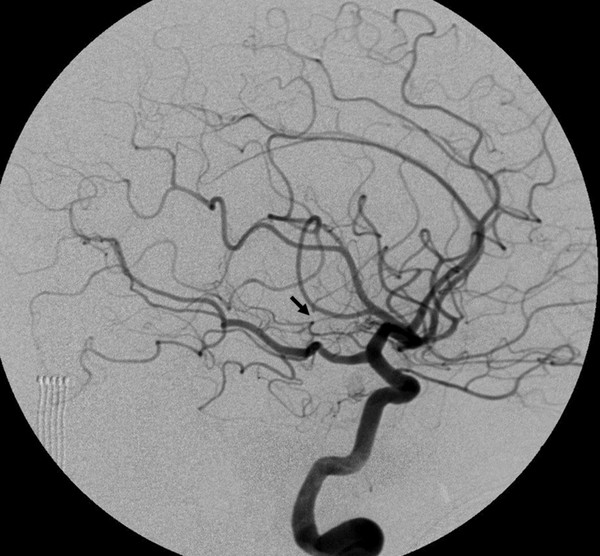
Fig. 9.2 Right ICA angiogram in lateral view demonstrates the AChoA arising cranial to the PcomA and coursing posteriorly toward the choroid fissure. The plexal (or choroidal point) is marked by a sharp curve, followed by a posterior turn (arrow). Note the prominent pituitary blush in this patient.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


