Abdominal Incision and Injection Sites
Michael P. Federle, MD, FACR
Harpreet Dhatt, BA
Key Facts
Imaging
Injection granulomas
Most common in subcutaneous fat of buttocks
Soft tissue or calcific density lesions
Injection site fluid or gas collection
Common in subcutaneous tissue of anterior abdominal wall (insulin, heparin, etc.)
Diabetic lipodystrophy
Insulin-dependent diabetic patients may develop atrophy or hypertrophy of fat at injection sites
Injection site lipohypertrophy (hypertrophy of fat and fibrous tissue)
Injection or incision site hematoma or seroma
May be misinterpreted as neoplastic mass
Injection or incision site abscess
Gas bubbles and enhancing wall with mass effect
Keloid (hypertrophic scar)
Overgrowth of tissue at site of healed skin injury
15x increased incidence in African-Americans
Calcified or ossified scar
May resemble rib, complete with cortex and medulla
Within linea alba after upper abdominal incision
Endometrial implantation in abdominal incision
Follows cesarean section or other uterine surgery
Cyclical pain at incision site with menstruation
Tumor implantation in incision sites
Can occur after “open” or laparoscopic incisions
Usually resembles primary tumor
Top Differential Diagnoses
Desmoid
Abdominal wall neoplasms
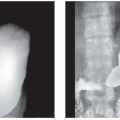
 (Left) Plain film radiograph shows rounded and linear calcified injection sites  within the subcutaneous fat overlying the buttocks. (Right) Axial CECT in the same patient shows the subcutaneous location and characteristic appearance of injection site granulomas within the subcutaneous fat overlying the buttocks. (Right) Axial CECT in the same patient shows the subcutaneous location and characteristic appearance of injection site granulomas  . . |
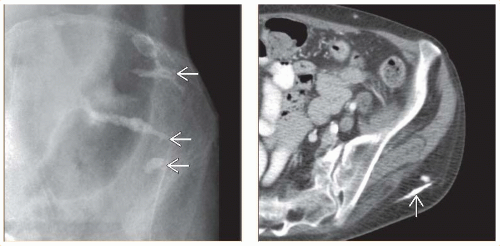
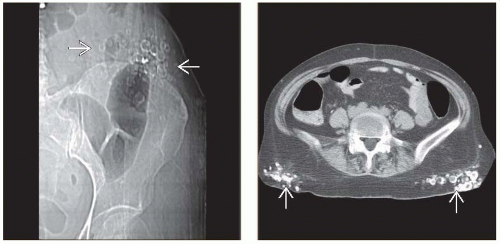 (Left) Plain film radiograph shows rounded calcifications  that overlap the lower abdomen. Some of these are lateral to the descending colon and close to the skin, establishing their extraabdominal location. (Right) Axial NECT in the same patient shows heavily calcified injection sites that overlap the lower abdomen. Some of these are lateral to the descending colon and close to the skin, establishing their extraabdominal location. (Right) Axial NECT in the same patient shows heavily calcified injection sites  in the subcutaneous tissues over the buttocks. Renal failure may have contributed to the deposition of so much calcium in these lesions. in the subcutaneous tissues over the buttocks. Renal failure may have contributed to the deposition of so much calcium in these lesions. |
TERMINOLOGY
Definitions
Lesions in abdominal wall or torso resulting from incision or injection sites; may be misinterpreted as other pathologic conditions
IMAGING
General Features
Best diagnostic clue
CT showing exact site and morphology of lesions
Size
Varies by etiology
Morphology
Varies by etiology
Imaging Recommendations
Best imaging tool
CT
Radiographic Findings
Injection granulomas
Soft tissue or calcific density lesions
Most common in subcutaneous fat of buttocks
More common with injection of alkaline solutions
Rarely within gluteal muscles
Though nurses have given “intramuscular” injections in buttocks for decades
Usually rounded; may be linear
May be misinterpreted as vascular, neoplastic, or inflammatory process within abdomen
May overlap lower abdomen
May simulate
Appendicolith
Ureteral calculus
Barium-lined diverticula
Atherosclerotic calcification
May be misinterpreted as sclerotic lesion in bones of pelvis
Key is to note change in position relative to bone on other radiographs
Easy to recognize on CT due to subcutaneous location and characteristic appearance
Injection site fluid or gas collection
Common in subcutaneous tissue of anterior abdominal wallRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree