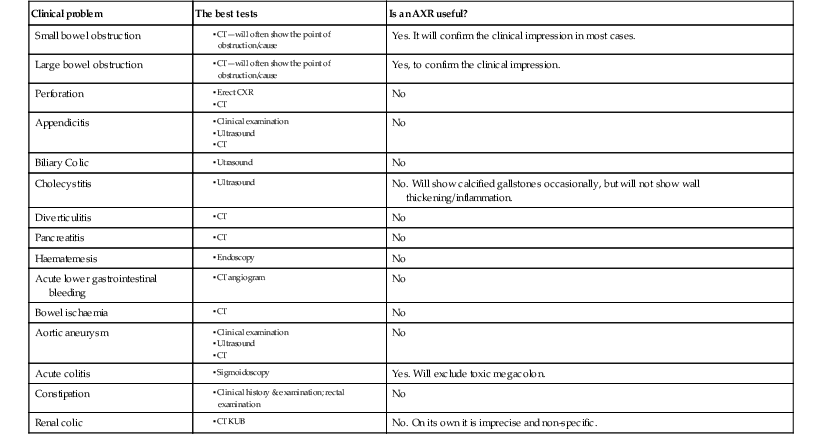
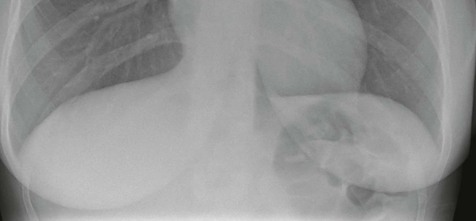
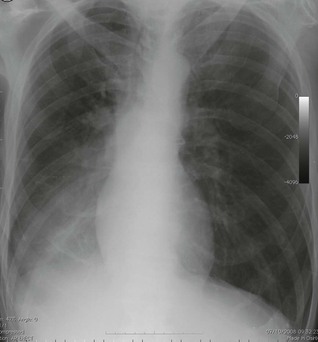
A patient with abdominal trauma does not require a plain abdominal radiograph (AXR). The AXR will not contribute to the clinical diagnosis and should be avoided. The AXR is of limited value as a diagnostic tool in the evaluation of many patients presenting with an acute abdomen. This is largely because the abdominal contents are composed of soft tissue. Plain film radiography does not provide adequate soft tissue contrast discrimination to detect and differentiate between many of the numerous inflammatory and neoplastic intra-abdominal soft tissue pathologies. The AXR is not the right tool for the job. Consequently, it has been superseded by ultrasound and CT scanning which are highly accurate in terms of evaluating the various intra-abdominal soft tissues. In present day clinical practice, the AXR is in the main limited to confirming a clinical suspicion of large or small bowel obstruction (as illustrated below), and demonstrating dangerous swallowed foreign bodies. Even so, CT will be selected as the first line imaging test in many cases of suspected intestinal obstruction, and also as the preferred and only imaging examination when renal colic is suspected. What if the preferrred imaging investigations are not immediately available? Is there any point in requesting an AXR as a substitute imaging test? On the whole, no. You risk obtaining false reassurance from a seemingly normal AXR appearance. It is safer to rely on a detailed clinical history and a careful physical examination. Furthermore, an experienced pair of examining hands from a member of the surgical team will recognise the emergency case that needs to go to theatre. The table on the right indicates the relatively few occasions when an AXR can be useful. Distended small bowel. No large bowel gas. Diagnosis: small bowel obstruction. Gross distention of the large bowel extending as low as the sigmoid colon. Diagnosis: large bowel obstruction. Radiology and abdominal pain ▪ CT ▪ CT ▪ CT ▪ CT KUB In the context of a patient attending the Emergency Department with abdominal pain there are just two questions to ask of the CXR: This erect CXR shows: normal lung bases and no free air under the diaphragm. The normal appearance of each lung is described on pp. 308–313. Abdominal pain. No specific diagnostic features from the history and clinical examination. The erect CXR reveals an extensive pneumonia in the right lower lobe. When analysing an AXR some normal features can be listed:
Abdominal pain & abdominal trauma
The AXR—its usefulness


Clinical problem
The best tests
Is an AXR useful?
Small bowel obstruction
Yes. It will confirm the clinical impression in most cases.
Large bowel obstruction
Yes, to confirm the clinical impression.
Perforation
No
Appendicitis
No
Biliary Colic
No
Cholecystitis
No. Will show calcified gallstones occasionally, but will not show wall thickening/inflammation.
Diverticulitis
No
Pancreatitis
No
Haematemesis
No
Acute lower gastrointestinal bleeding
No
Bowel ischaemia
No
Aortic aneurysm
No
Acute colitis
Yes. Will exclude toxic megacolon.
Constipation
No
Renal colic
No. On its own it is imprecise and non-specific.
Analysis: plain film checklists
Erect CXR
Supine AXR

Abdominal pain & abdominal trauma
19








