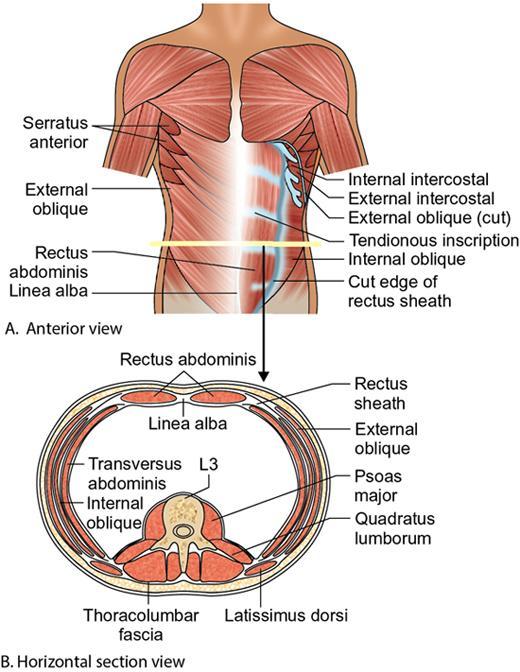
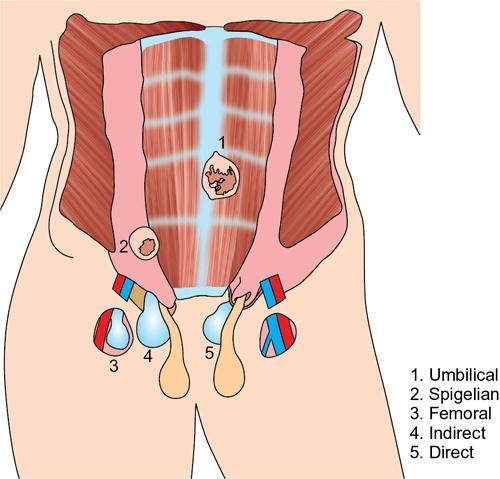
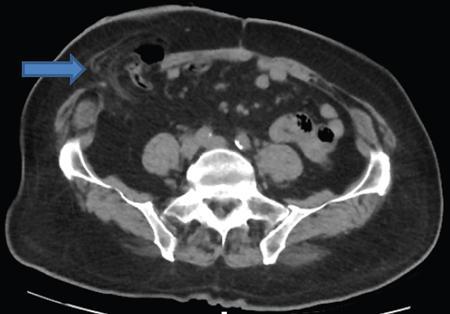
Amandeep Singh The abdominal wall surrounds the anterolateral aspect of the abdominal cavity, where many important organs are located. The abdominal wall is made up of: Superior epigastric artery, inferior epigastric artery, deep circumflex iliac vessels, superficial epigastric vessels and superficial circumflex iliac vessels supply the anterior abdominal wall. Nerves of the anterior abdominal wall include subcostal nerve, iliohypogastric and ilioinguinal nerves. Types of abdominal hernias: The diagnosis of hernia can be made with plain radiographs, barium studies and CT. They consist of a peritoneal sac which protrudes through a weakness/defect in the muscular layers of the abdominal wall (mainly in transversalis fascia below the conjoined tendon). Preperitoneal fat, greater omentum and viscera may protrude into the sac (Fig. 7.15.2). Types: Indirect or direct (depending on their relationship to the inferior epigastric vessels). Indirect hernia: They occur in infants and children. The peritoneal sac passes through the internal ring into inguinal canal, lateral to the inferior epigastric vessels and anterior to the spermatic cord. In women, it goes along the round ligament into the labium. Rarely, the herniated sac instead of leaving the external inguinal ring continues along with the abdominal wall muscles. This is called interparietal hernia (Fig. 7.15.3). Direct hernia: It is always acquired. The herniated sac is medial to the inferior epigastric vessels and does not pass through the inguinal canal. Hence, they do not reach up to scrotum. Femoral hernias are less common than inguinal hernias. They are more common in paediatric age groups and women. The predisposing feature is the empty space between the lacunar ligament medially and the femoral vein laterally. Physical changes of pregnancy dilate this space. The herniated sac is below the inguinal ligament and lateral to the femoral vessels. Strangulation is a common complication. In femoral hernia, the sac lies below and lateral to the pubic tubercle as it emerges from the femoral canal. It can be differentiated from an inguinal hernia which lies above and medial to the pubic tubercle (Fig. 7.15.4). Incisional hernias occur as a result of complication of laparotomy. Risk factors include old age, obesity, postoperative wound infection, chronic pulmonary disease, cirrhosis, malignant tumour, steroids and malnutrition. Most of these hernias develop during the first few months after surgery but may remain silent for up to a period of 5 years. Incisional hernia are more likely to occur as a result of vertical incisions than transverse incisions. They may occur following incisions as small as a puncture site for laparoscopic surgery. A common variation is the parastomal hernia, in which bowel and omental fat protrude through a defect immediately adjacent to an ileostomy or colostomy opening. Bowel loops may be incorporated into the hernia and become incarcerated or strangulated, if the hernia is not treated (Fig. 7.15.5). Richter’s hernia is a rare type of hernia which includes only a part of the bowel wall. Because only a portion of the intestinal wall is included into the hernia, therefore, the lumen remains patent and does not result in obstruction. However, incarceration is not common. Any hernia which contains a Meckel’s diverticulum is known as Littre hernia. They may occur due to the presence of inflammatory adhesions that cause confinement of the Meckel’s diverticulum within the hernia sac. Approximately 50% of Littre hernias develop in the inguinal region, 20% in the femoral, 20% in umbilical and 10% in other sites. Spigelian hernia is a rare acquired ventral hernia that occurs through the linea semilunaris, the line where lateral rectus sheath is formed by fusion of sheaths of lateral abdominal muscles. They are almost always found just above the point where posterior wall of the rectus sheath is pierced by the inferior epigastric vessels. It occurs at midpoint between the umbilicus and symphysis pubis, which is a weak point along the lateral border of the rectus muscle. They are rare but have a high frequency of incarceration and strangulation. It may be mistaken for an abdominal wall lipoma, if it contains only peritoneal fat. CT can be quite beneficial to confirm the diagnosis (Fig. 7.15.6).
7.15: Abdominal wall pathologies and hernias
Introduction
Blood supply
Nerve
Hernias
External hernias
Inguinal hernias
Femoral hernias
Incisional hernias

Richter’s hernias
Littre hernias
Spigelian hernias
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


