Upper GI tract
Erosion ulcer
Variceal bleeding
Mallory-Weiss tear
Vascular lesions
Neoplasms
Lower GI tract
Diverticular disease
Angiodysplasia
Neoplasms
Colitis
Benign anorectal lesions
Imaging Techniques
Since endoscopic localization and control of luminal bleeding has become the mainstay of management, a gastroenterology evaluation should be obtained early in the course of bleeding. However, endoscopic techniques only work if the bleeding lesion can be adequately visualized. Urgent colonoscopy has been shown to identify a bleeding site in only 13 % of patients and a probable bleeding site in 67 % despite adequate colon preparation.
Catheter-directed angiography has been shown to have high sensitivity and 100 % specificity for upper and lower GI bleeding, however it is dependent on the presence of bleeding. When present, bleeding rates as low as 0.5 ml/min can be detected.
CT angiography has shown promising results with sensitivity and specificity for detecting and localizing GI bleeding of over 90 %.
If cirrhosis and variceal bleeding is a consideration, then LFT or bedside ultrasound to assess for ascites might also be useful.
Barium studies have no role for acute GI bleeding investigation (upper or lower) and will only obscure details at endoscopy, place the patient at risk for aspiration, and consume valuable time.
Upper GI Bleeding
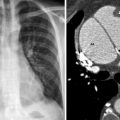
Upper endoscopy is the therapy of choice in these cases, offering both diagnosis and treatment options, and should be employed early in the course. If non-variceal bleeding is identified various ways to stop the bleeding, such as epinephrine injection, thermal coagulation, or hemoclip application, have all been utilized. Angiography with embolization can be used as an adjunct (Fig. 32.1a, b). When angiography is used for therapy the options include embolization, which is not necessarily intended to be permanent (Gelfoam or similar) or efforts at permanent closure with either mechanical agents (microcoils) or chemical agents (such as polyvinyl alcohol, NBCA glue, etc.). Infusion of a constrictive agent such as vasopressin can also be delivered intra-arterially via this route, but seems to be associated with higher failure rates and has the additional potential complications of local tissue necrosis or systemic effects such as myocardial ischemia.