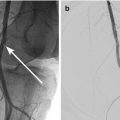
Fig. 31.1
(a) Ultrasound of right kidney shows dilated pelvicalyceal system in keeping with hydronephrosis. (b) Fluoroscopic image following insertion of a percutaneous nephrostomy shows contrast medium within the decompressed pelvicalyceal system
Doppler ultrasonography can be used to evaluate renal blood flow to exclude hypoperfusion or venous congestionas a cause of AKI. It has to be remembered though, that renal blood flow is reduced in both prerenal and intrarenal AKI, limiting the diagnostic utility of Doppler ultrasonography in patients with AKI.
Computed Tomography
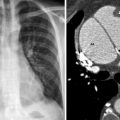
Standard intravenous nonionic iodinated contrast medium used for CT is potentially nephrotoxic (see Chap. 12) and should be avoided whenever possible to minimize compounding existing renal insults. CT without intravenous contrast material can identify dilation in the renal collecting system and may be helpful in evaluating for obstruction in patients where sonography is technically limited. It may also help to identify other extra-renal conditions, such as an intra-abdominal abscess (see Chap. 29), which may be associated with AKI. Non-contrast enhanced CT may be invaluable in planning operative intervention by providing information about the peritoneal as well as retroperitoneal anatomy. CT can readily identify direct renal injuries and their sequelae including intra-renal hemorrhage, renal contusion and surrounding hematoma (Fig. 31.2). Missed injuries such as a renal pelvis injury (Fig. 31.3a, b), which will not show any ureteral dilatation because the ureter is decompressed, show up as urinoma on CT.