Acute Multiple Sclerosis Flare
Shaun R. Wagner
CLINICAL HISTORY
37-year-old male presents with new onset of extreme leg weakness and memory issues.
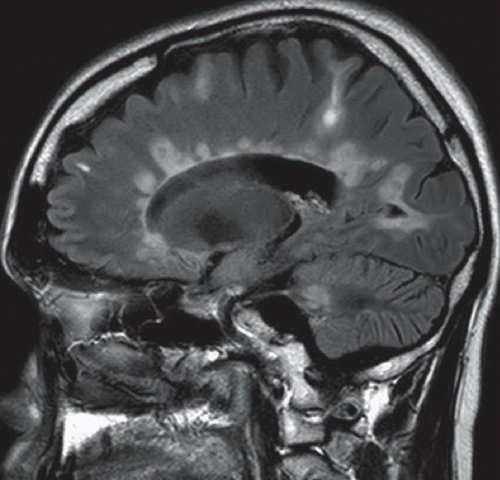 FIGURE 85A |
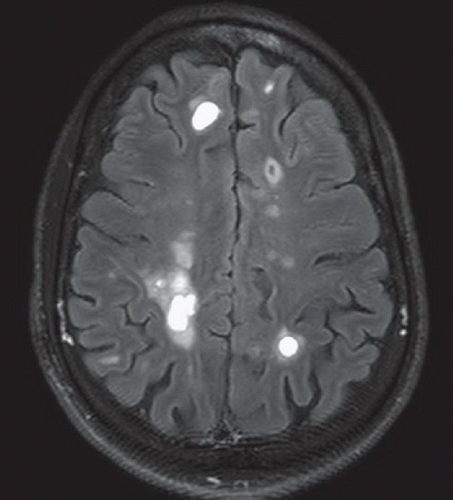 FIGURE 85B |
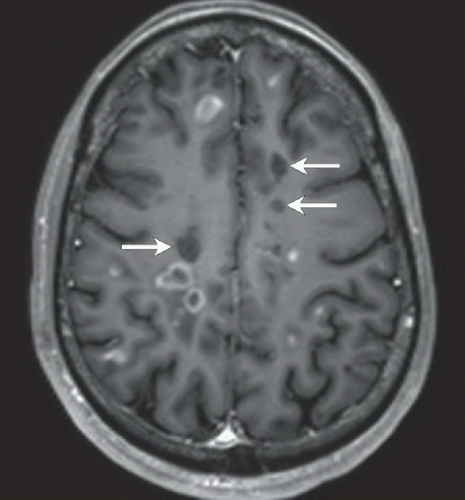 FIGURE 85C |
FINDINGS
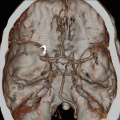
Figure 85A: Sagittal FLAIR image slightly to the left of midline demonstrates numerous hyperintense white matter lesions, many of which are adjacent to the lateral ventricle and oriented perpendicular to the callosal-septal margin. There is prominence of the sulci compatible with cerebral volume loss. Figure 85B: Axial FLAIR image just superior to the lateral ventricles demonstrates extensive hyperintense lesions within the centrum semiovale and juxtacortical white matter. Figure 85C: Axial postcontrast T1 image demonstrates both peripheral and solid enhancement of a number of the white matter lesions. Notice that the enhancing lesions correspond to some of the most brightly hyperintense lesions on FLAIR imaging. Note also the hypointense lesions within the bilateral frontal lobes (arrows) consistent with “black holes,” indicating myelin/axonal loss.
DIFFERENTIAL DIAGNOSIS
The findings in this case are characteristic of an acute flare of multiple sclerosis (MS), but a number of other entities can produce white matter lesions on imaging. On the benign end of the spectrum, chronic leukoaraiosis and migraine headaches could be included in the differential for MS. Leukoaraiosis is typically seen in older patients, often in association with long-standing hypertension, and the lesions in this entity do not enhance. Patients younger than 40 years suffering from migraines may demonstrate T2 hyperintense foci, predominantly within the subcortical white matter. These lesions have a frontal and parietal lobe predilection and are stable over time. Virchow-Robin (VR) spaces are dilated perivascular spaces containing CSF. Common locations for VR spaces include the basal ganglia, centrum semiovale, and corona radiata. They may simulate MS plaques on MR in
that they will demonstrate T1 hypointensity and T2 hyperintensity, but will appear hypointense on FLAIR imaging because of CSF within these spaces, which differentiates them from MS plaques. In the setting of multiple enhancing lesions, one might consider multiple brain metastases. Generally most metastases will enhance, whereas only active plaques will enhance in multiple sclerosis. In addition, brain metastases tend to demonstrate varying degrees of peripheral vasogenic edema, whereas MS plaques do not. Acute disseminated encephalomyelitis (ADEM) may also be in the differential of multiple T2 hyperintense lesions within the white matter. Lesions in ADEM range from punctate to quite large and typically do not involve the callosal-septal interface. ADEM occurs most commonly in children and typically follows a minor viral infection or immunization.
that they will demonstrate T1 hypointensity and T2 hyperintensity, but will appear hypointense on FLAIR imaging because of CSF within these spaces, which differentiates them from MS plaques. In the setting of multiple enhancing lesions, one might consider multiple brain metastases. Generally most metastases will enhance, whereas only active plaques will enhance in multiple sclerosis. In addition, brain metastases tend to demonstrate varying degrees of peripheral vasogenic edema, whereas MS plaques do not. Acute disseminated encephalomyelitis (ADEM) may also be in the differential of multiple T2 hyperintense lesions within the white matter. Lesions in ADEM range from punctate to quite large and typically do not involve the callosal-septal interface. ADEM occurs most commonly in children and typically follows a minor viral infection or immunization.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


