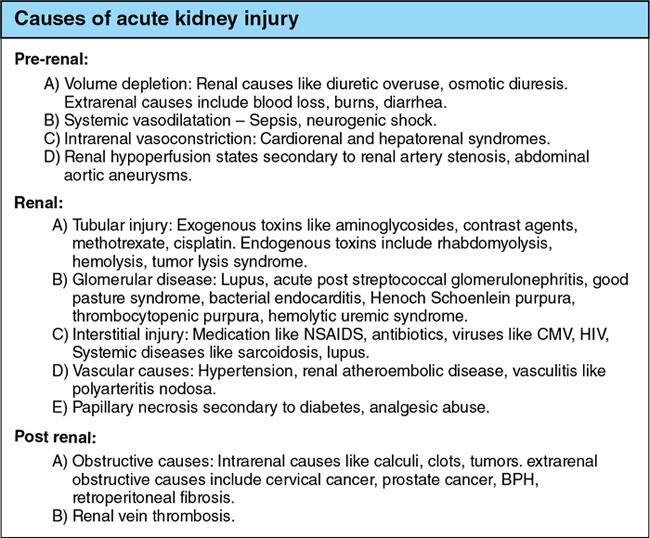
Acute kidney injury (AKI) is a heterogeneous syndrome which is defined as a decline in the glomerular filtration rate rapidly (hours to days) leading to retention of waste products like urea and creatinine, further resulting in dysregulation of electrolytes, fluid, homeostasis of acid-base. The term acute renal failure (ARF) is now replaced by AKI indicating substantial clinical importance of smaller decrements in kidney function which do not result in overt organ failure and are associated with increased mortality and morbidity. AKI is defined as any of the following – urine volume <0.5 mL/kg/h for 6 hours or increase in serum creatinine 1.5 times baseline which is known or occurred presumably within the prior 7 days or increase in serum creatinine within 48 hours by >0.3 mg/dL. AKI categorized depending upon the 24-hour urine output: AKI is the internationally preferred term to replace acute renal failure. Renal function is most often assessed by serum creatinine. Creatinine levels may be falsely high in patients with decreased muscle mass and poor nutritional status. Glomerular filtration rate (GFR) is the overall preferred measure of renal function. Loss of renal function may be temporary and reversible with less than 20% of cases requiring renal replacement therapy. Imaging plays an important role in identifying correctable causes of renal failure. For diagnostic and therapeutic purposes, the causes of ARF are divided into three broad categories summarized in Fig. 10.12.3.2.1: Most patients with AKI will have either a prerenal or renal cause for AKI with only 10%–15% having a postrenal aetiology. Imaging is vital in diagnosing these 10%–15% which are often correctable and reversible. Clinical overlap is common in acute renal failure. A complete evaluation requires a combination of clinical assessment, laboratory findings and histopathology to arrive at a correct diagnosis. The role of imaging in renal failure is to segregate the surgical and medical conditions resulting in renal insufficiency and to identify correctable causes of renal failure like obstruction, renal vein thrombosis and renal artery stenosis. Another important role of imaging in the initial assessment is to estimate size of the kidneys which helps differentiate acute from chronic renal parenchymal disease. Imaging in particular ultrasound is also helpful in follow up of cases of acute renal failure to assess for resolution or progression. Radiographs depict renal calculi and parenchymal calcification. They can also be used for preliminary assessment of size. Renal contour and size can be estimated if the outlines are well seen. Renal size is approximately equal to the height of 3–4 lumbar vertebrae. Discrepancy in renal size of more than 2 cm is considered significant. In the present era, the role of intravenous urography (IVU) in assessing renal abnormalities has significantly reduced. Besides in the setting of acute renal shut-down, it is unwise to administer intravenous contrast agents which are nephrotoxic unless necessary. Characteristic abnormal patterns have been described by Fry and Cattell: In patients with AKI, a radiograph or noncontrast CT may show a bilaterally symmetrical, dense, prolonged nephrogram due to contrast administered for a previous examination. Ultrasound is the initial imaging modality preferred for acute renal failure given its ease of use, safety profile, accessibility and noninvasive nature. The American College of Radiology Appropriateness Criteria gives ultrasound the highest rating of 9/10 in the initial evaluation of AKI. Although only 10% of ultrasound examinations demonstrate abnormal findings related to AKI, it has a significant impact on patient management. A normal ultrasound helps in guiding management by excluding obstructive causes and major structural abnormalities. The following features are assessed on ultrasound: Numerous studies have established the normal renal length to range from 9 to 12 cm. Renal size and parenchymal thickness evaluation are helpful in assessing chronicity of disease. Small-sized kidneys are usually seen in chronic renal failure in which recovery is unlikely. In AKI the kidneys are of normal size or enlarged. Enlarged kidneys are seen in acute interstitial nephritis and acute tubular necrosis. Infiltrative disease processes like lymphoma and myeloma, infective causes like pyelonephritis, nephrotic/nephritic syndromes and renal vein thrombosis also result in bilateral enlarged kidneys. In AKI the kidneys maintain a smooth contour. Renal parenchymal thickness is measured as the distance between the interpapillary line and the lateral renal cortex. It is usually around to 2.5–3 cm. Reduction is seen in renal parenchymal loss while an increase in renal parenchymal thickness is seen in infiltrative diseases. Parenchymal thickness can help differentiate acute from chronic renal disease. Chronic kidney disease results in decreased parenchymal thickness. Bilateral involvement of kidneys indicates systemic causes. Renal parenchymal echogenicity is normally less than that of the liver and spleen. An increased or altered echogenicity suggests renal parenchymal disease. Renal corticomedullary differentiation may be normal, obliterated or increased. If cortical echogenicity is increased with maintained corticomedullary differentiation, infiltrative diseases like glomerulonephritis, amyloidosis, acute leukaemia and Alport’s syndrome are to be considered. Reduced cortical echogenicity is seen in lymphoma, acute pyelonephritis and renal vein thrombosis. Increased medullary echotexture is found in gouty nephropathy, medullary nephrocalcinosis and medullary sponge kidney. Hydration status at the time of scan may alter the cortical and medullary echotexture and hence the corticomedullary differentiation. An extracapsular hypoechoic rim of oedema may surround the kidneys in renal failure. This finding is usually bilateral and is called the ‘kidney sweat sign’. Ultrasound is the initial imaging modality used to detect obstruction of the renal collecting system, ureters or bladder. Dilatation of the pelvicalyceal system/ureters, bladder distension or wall thickening, presence of calculi, prostate enlargement or extrinsic causes of obstruction like pelvic or retroperitoneal malignancies must be assessed carefully. These are important to diagnose because treatment depends upon relieving the obstructing cause and preserving renal function. Ultrasound in ARF (Fig. 10.12.3.2.2):
2. Acute renal failure
Introduction
Aetiology
Role of imaging
Imaging techniques
Plain radiograph (KUB)
Intravenous urography
Ultrasonography
Laterality
Parenchymal echogenicity
Corticomedullary differentiation
Extracapsular signs
Signs of obstruction/hydronephrosis
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


