Acute Right MCA Occlusion—“Dense MCA” Sign
Parth C. Patel
CLINICAL HISTORY
23-year-old male with sudden onset of left arm weakness, left facial droop, and dysarthria.
 FIGURE 45A |
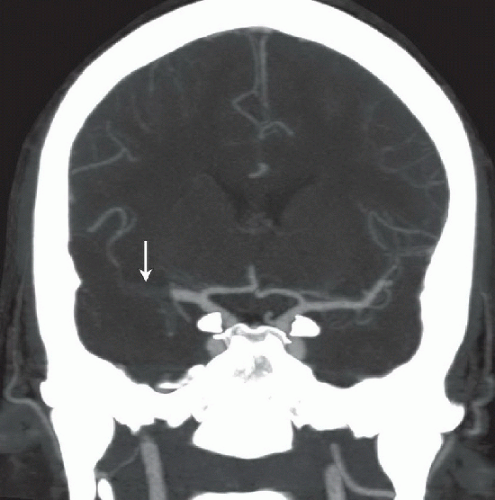 FIGURE 45B |
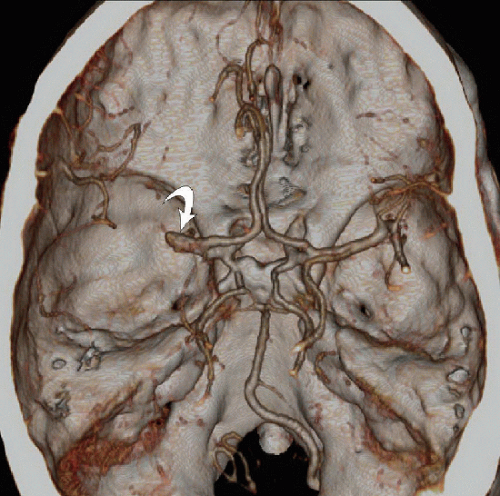 FIGURE 45C |
FINDINGS
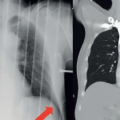
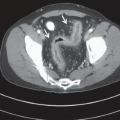
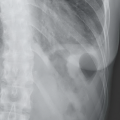
Figure 45A: Axial noncontrast enhanced CT image reveals increased density (arrowheads) of the M1 segment of the right middle cerebral artery (MCA). No obvious parenchymal hypodensity or hemorrhage is present. Figure 45B: Coronal thick MIP image from a CT angiogram of the circle of Willis demonstrates an occlusive filling defect in the lateral half of the right M1 segment (arrow) extending into the proximal M2 branches. Figure 45C: 3D surface shaded reconstruction from the CTA again demonstrates occlusion of the right MCA. The curved arrow indicates the proximal stump of the right MCA.
DIFFERENTIAL DIAGNOSIS
In this particular case, there is no real differential. The primary diagnostic consideration given the history and imaging findings is an acute stroke caused by thromboembolic occlusion of the right MCA. Entities that can produce hyperdensity of the MCA on unenhanced CT imaging include high hematocrit, usually from dehydration, high atherosclerotic burden, partial volume averaging, recent administration of intravenous contrast, and very rarely herpes simplex encephalitis. Recognizing these false positives can have great implications on patient management and outcome, especially in the recombinant-tissue plasminogen activator (t-PA) era. In this case, the CTA findings are diagnostic of MCA occlusion.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


