Acute Subdural Hematoma
Kwaku A. Obeng
CLINICAL HISTORY
65-year-old female who became unresponsive after a fall at home. On arrival at the ED, the patient was noted to have nonreactive pupils with weak corneal reflexes and absent cough and gag reflexes.
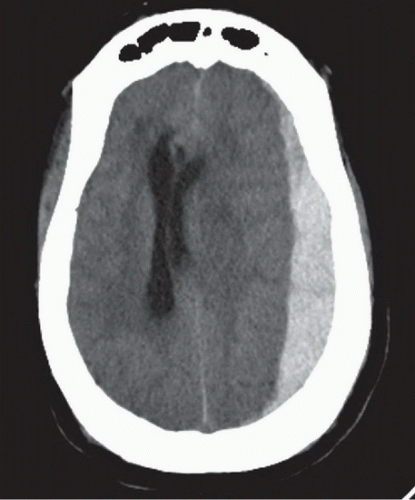 FIGURE 49A |
 FIGURE 49B |
 FIGURE 49C |
FINDINGS
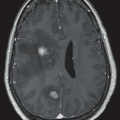
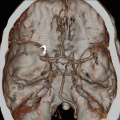
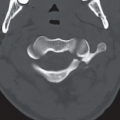
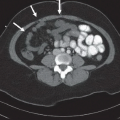
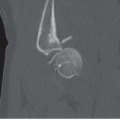
Figures 49A,49B and 49C: Axial noncontrast head CT images from superior to inferior demonstrate a hyperdense, crescentic extra-axial fluid collection extending along the left cerebral convexity. The collection crosses suture lines, but does not extend across the midline dural reflections. There is significant mass effect, evidenced by rightward shift of the lateral ventricles and third ventricle (arrow in Fig. 49B), indicating subfalcine herniation. In addition, in Figure 49C, the ambient and quadrigeminal cisterns are completely effaced, and the left uncus (arrowhead) appears to extend medially over the expected location of the left tentorial incisura, suggesting downward transtentorial herniation. Large right-sided periorbital hematomas are also evident on Figures 49B and 49C.
DIFFERENTIAL DIAGNOSIS
The above findings are pathognomonic of an acute subdural hematoma (SDH) with associated subfalcine and uncal herniation. The differential diagnosis for a subdural collection is based mostly on the CT attenuation or MR intensity of the collection. Increased density of the collection relative to the adjacent brain parenchyma indicates hemorrhage. In the setting of trauma, an acute SDH needs to be distinguished from an epidural hematoma. The latter type of hemorrhage is typically biconvex in appearance, contained by the sutures, and often has an associated overlying calvarial fracture. Epidural
hematomas can also cross dural reflections, whereas SDHs are limited by them.
hematomas can also cross dural reflections, whereas SDHs are limited by them.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


