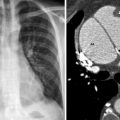
Fig. 30.1
Longitudinal transabdominal ultrasound image of the right upper quadrant shows hypoechoic hemorrhage (arrows) anterior to the liver and in the hepatorenal fossa. Hyperdense acute hemorrhage (open arrow) is also seen in the hepato-renal fossa
Ultrasound
Ultrasound is highly sensitive in detecting free peritoneal fluid in the abdomen or pelvis (Fig. 30.1). It is portable, inexpensive, and provides the opportunity for diagnostic aspiration or therapeutic drainage of collections and is therefore well suited to the ICU setting. Ultrasound may be limited due to dressings, bowel gas or patient body habitus and is less sensitive in detecting retroperitoneal hematoma.
Plain Radiograph
If the patient had a central venous catheter (CVC) placed in the internal jugular vein or the subclavian vein preoperatively, a CXR will evaluate for a hemothorax as a potential source of blood loss. Another very rare complication after CVC placement is cardiac tamponade. Although clinical signs will likely lead to patient instability long before a change in labs, the CXR may show a change in heart size or shape, leading one to suspect a problem. Use of ultrasound guidance for placement of these catheters has decreased the complications but does not eliminate them.
There is no indication for an abdominal plain film (flat plate or upright) in the evaluation of postoperative decrease in hemoglobin or suspected postoperative intraabdominal bleeding. Sitting the patient up or putting them in a lateral position carries a high risk of further hemodynamic destabilization. Plain films of the abdomen allow for evaluation of pneumoperitoneum or intraluminal air. They are not helpful for the evaluation of extraluminal blood.
Computed Tomography
In the acute setting CT is useful for the detection of a large number of post-operative complications, including bleeding, perforation, abscess, fluid collections, wound dehiscence, bowel obstruction and anastomotic leak. If the location of bleeding is unrelated to the surgical site and is away from the drains, such as the retroperitoneum or the abdominal wall, a CT can guide the diagnosis and save valuable time (Figs. 30.2 and 30.3). CT assessment of fluid attenuation also allows for differentiation between ascites (0–20 HU) and blood (30–70 HU) in the peritoneal cavity. Acute intraabdominal bleeding can mimic ascites on a postoperative CT, particularly in the presence of profound anemia and large-volume crystalloid resuscitation. Narrow CT window settings (window center = 70; window width = 300) facilitate visualization of a fluid-fluid level with more dense dependent sedimented red blood cells. This finding, known as the “hematocrit effect,” was initially described in anticoagulated patients but is also useful for detecting subtle hemorrhage (Fig. 30.4).