Added Benefits of PET/CT
Todd M. Blodgett, MD
Alex Ryan, MD
Hesham Amr, MD
Added Benefits of PET/CT Imaging
Technical Benefits
Consolidation of patient’s imaging studies
More convenient to patients
Imaging times reduced by up to 40% compared to dedicated PET alone
Transmission scans do not need to be performed with PET/CT
CT used for attenuation correction
Easy integration with radiation therapy planning
Clinical Benefits
Detection of lesions by PET not detected on CT, even with good contrast enhancement on CT
Detection of lesions within streak artifact or beam hardening artifact on CT
Improved lesion localization when images are accurately coregistered, particularly when no definite abnormality on CT
Improved biopsy localization information
Improved radiation therapy planning
Exclusion of suspicious lesions on other imaging modalities
Improved differentiation of physiologic from pathologic FDG activity
Summary of PET/CT Literature
Most comparative studies of PET or CT vs. combined PET/CT have shown incremental benefit of having accurately coregistered images
PET/CT often has clinical impact and leads to changes in clinical management
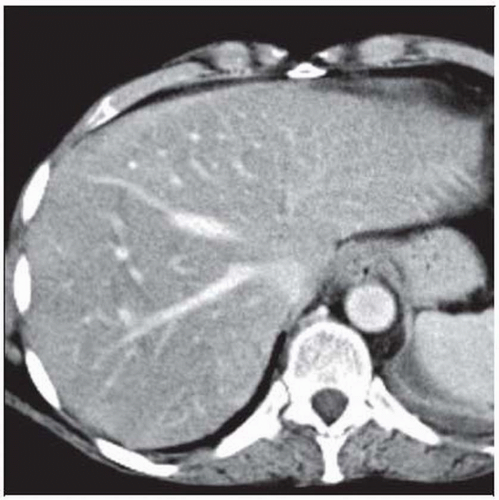 Axial CECT (with well-timed portal venous phase) of a patient with a history of breast cancer and recent rise in CA 27-29 shows no evidence of hepatic lesions. |
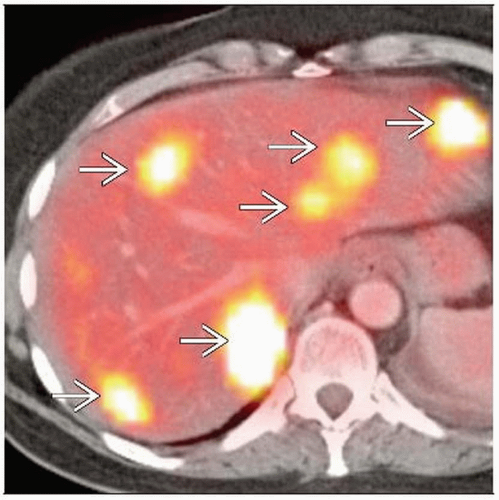 Axial fused PET/CT shows at least 6 FDG-avid bilobar hepatic metastatic lesions  . One of the major added benefits of PET/CT is detection of lesions not identifiable on CT, even with good contrast enhancement. . One of the major added benefits of PET/CT is detection of lesions not identifiable on CT, even with good contrast enhancement. |
TERMINOLOGY
Abbreviations
PET/CT benefits
Definitions
Benefits of hardware PET/CT fusion
CLINICAL IMPLICATIONS
Clinical Importance
Most comparative studies of PET or CT vs. combined PET/CT have shown incremental benefit of PET/CT
Often affect clinical management
Often reduce indeterminate lesions
GENERAL CONSIDERATIONS
DICOM Fusion Methods
Mental fusion
Side-by-side inspection of PET and CT images and visual fusion
Least effective method, unless lesion is obvious on both CT and PET
Retrospective software coregistration
Several proprietary software programs to register two DICOM data sets
Even data acquired at different times on different scanners can be coregistered
Tend to work well with brain applications, including coregistration of PET and MR
Brain is fixed in position by the skull; therefore, coregistering two independent data sets is relatively accurate
Less reliable in whole-body applications due to differences in patient positioning, internal organ movement, and technique differences
Software registration fails where it could be the most useful
When there is a lesion on PET not visualized or present on CT
Hardware fusion
Hardware fusion increases confidence level of interpreting physician for accurately localizing a lesion not visible on CT
Provides optimal coregistration of PET and CT images acquired in one imaging session
If patient moves between PET and CT portions of exam, images will have inaccurately coregistered images
Data is acquired sequentially rather than simultaneously
Motion restraint devices recommended
TECHNICAL ADDED BENEFITS
Decrease in Total Scan Time
Approximately 40% less time to do PET and CT on a combined PET/CT scanner than to acquire PET and CT on a dedicated PET scanner and CT scanner
For a typical scan protocol, emission scan takes 2-5 minutes/bed position, for a total emission time of 12-30 minutes for a 6-bed-position scan
Total scan times for hardware PET/CT: Emission scan time (˜ 12-30 mins) + CT scan time (1-3 minutes)
No need to perform a separate transmission scan on hardware PET/CT, as CT is used for attenuation correction
Transmission scan performed on a dedicated PET scanner adds 12-24 minutes to the overall scan time
Consolidation of Imaging Studies
Prior to PET/CT, patients usually scanned on separate PET and CT scanners, usually in different departments or even different hospitals
As most patients have CT scans when first diagnosed with malignancy, performing PET and CT in single scanning session is optimal
Radiation Therapy Planning Integration
Many patients with newly diagnosed malignancies will be candidates for radiation therapy planning
PET and CT DICOM data sets can be imported into almost all major planning software systems
Obviates the need for separate planning CT as long as the patient is positioned with flat “radiation therapy planning” bed
CLINICAL ADDED BENEFITS
General Added Benefits of PET/CT
Detection of lesions by PET missed on CT, even with good contrast-enhanced CT
Contrast-enhanced CT more sensitive than noncontrast CT but still may miss early lesions, even with good parenchymal enhancement
CT very insensitive for detection of early lytic bone metastases; FDG PET more sensitive than traditional bone scanning for detection of osteolytic lesions
For CMS covered indications, FDG PET has a higher sensitivity than CT alone for most applications
Detection of Lesions in CT Artifacts
Fused PET/CT images allow confident detection and localization of a lesion that may be obscured by streak artifacts on CT
Improved Lesion Localization
Reliance on accurate coregistration is essential
Fused PET/CT images show the location of the lesion despite an anatomical abnormality on CT
Biopsy Localization Information
Can identify the most metabolically active portion of a lesion
Can minimize sampling error
Improved Radiation Therapy Planning
Usually leads to decrease in gross tumor volume (GTV) and clinical tumor volume (CTV) in patients with central lung cancers and post-obstructive atelectasis by identifying tumor margins more accurately
Usually leads to increase in GTV in planning for other tumors by identifying unsuspected additional lesions
Exclusion of Suspicious Lesions
Patients often referred for further evaluation of a suspicious lesion on ultrasound, CT, or MR
PET/CT can help exclude possible malignancy
Physiologic vs. Pathologic FDG Activity
Prior to PET/CT, areas of focal muscular FDG activity and brown fat were often misinterpreted as pathology
Many structures may have intense physiologic FDG activity
PET/CT helps differentiate physiologic from pathologic FDG activity by allowing accurate coregistration
BRIEF REVIEW OF LITERATURE
General Oncology
Comparative studies of PET/CT vs. PET and CT side-by-side
Fewer equivocal interpretations due to enhanced observer confidence
Most studies show PET/CT has modest but clinically relevant impact on diagnostic performance
PET/CT provides additional information in 41-49% of patients compared to visually correlated PET and CT
Significantly more accurate than CT alone, PET alone, and visually correlated PET and CT for T staging
Shown to have accuracy for TNM staging superior to other modalities
Accuracies of 84% for PET/CT, 76% for side-by-side, 63% for CT alone, and 64% for PET alone
PET/CT impact on patient management
Head and Neck Cancer
Receiver operating characteristic curve (ROC) analyses demonstrated that PET/CT was significantly better than FDG PET or CT alone for depiction of malignancy in the head and neck
Sensitivity and specificity
PET/CT: 98% and 92%
PET alone: 87% and 91%
CT alone: 74% and 75%
Accuracy, PPV, NPV
PET/CT: 94%, 88%, 99%
PET alone: 90%, 85%, 92%
CT alone: 74%, 63%, 83%
Colorectal Cancer
Certainty of lesion localization and characterization: Major improvement with the combined modality
PET/CT reduced number of lesions of uncertain location by 55% and number of equivocal and probable lesion characterizations by 50%
Sensitivity, specificity, accuracy
PET/CT: 86%, 67%, 83%
PET: 88%, 56%, 83%
Major advantage of PET/CT over PET is in overall improved staging accurately
Number of patients incorrectly staged was reduced by half with PET/CT
Overall accuracy of staging increased from 78% to 89%
RELATED REFERENCES
1. Benz MR et al: Treatment Monitoring by 18F-FDG PET/CT in Patients with Sarcomas: Interobserver Variability of Quantitative Parameters in Treatment-Induced Changes in Histopathologically Responding and Nonresponding Tumors. J Nucl Med. 49(7):1038-1046, 2008
2. Farma JM et al: PET/CT fusion scan enhances CT staging in patients with pancreatic neoplasms. Ann Surg Oncol. 15(9):2465-71, 2008
3. Ford EC et al: Comparison of FDG-PET/CT and CT for delineation of lumpectomy cavity for partial breast irradiation. Int J Radiat Oncol Biol Phys. 71(2):595-602, 2008
4. Gjelsteen AC et al: CT, MRI, PET, PET/CT, and ultrasound in the evaluation of obstetric and gynecologic patients. Surg Clin North Am. 88(2):361-90, vii, 2008
5. Hillner BE et al: Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone on expected management of patients with cancer: initial results from the National Oncologic PET Registry. J Clin Oncol. 26(13):2155-61, 2008
6. Kitajima K et al: Performance of integrated FDG-PET/contrast-enhanced CT in the diagnosis of recurrent ovarian cancer: comparison with integrated FDG-PET/non-contrast-enhanced CT and enhanced CT. Eur J Nucl Med Mol Imaging. 35(8): 1439-48, 2008
7. Kuehl H et al: Impact of whole-body imaging on treatment decision to radio-frequency ablation in patients with malignant liver tumors: comparison of [18F]fluorodeoxyglucose-PET/computed tomography, PET and computed tomography. Nucl Med Commun. 29(7):599-606, 2008
8. Murakami R et al: Impact of FDG-PET/CT fused imaging on tumor volume assessment of head-and-neck squamous cell carcinoma: intermethod and interobserver variations. Acta Radiol. 49(6):693-9, 2008
9. Schreurs LM et al: Better assessment of nodal metastases by PET/CT fusion compared to side-by-side PET/CT in oesophageal cancer. Anticancer Res. 28(3B):1867-73, 2008
10. Tikkakoski T: Impact of FDG-PET/CT fused imaging on tumor volume assessment of head-and-neck squamous cell carcinoma. Acta Radiol. 49(6):615-6, 2008
11. Weigert M et al: Whole-body PET/CT imaging: combining software- and hardware-based co-registration. Z Med Phys. 18(1):59-66, 2008
12. Casneuf V et al: Is combined 18F-fluorodeoxyglucose-positron emission tomography/computed tomography superior to positron emission tomography or computed tomography alone for diagnosis, staging and restaging of pancreatic lesions? Acta Gastroenterol Belg. 70(4):331-8, 2007
13. Branstetter BF 4th et al: Head and neck malignancy: is PET/CT more accurate than PET or CT alone? Radiology. 235(2):580-6, 2005
Image Gallery
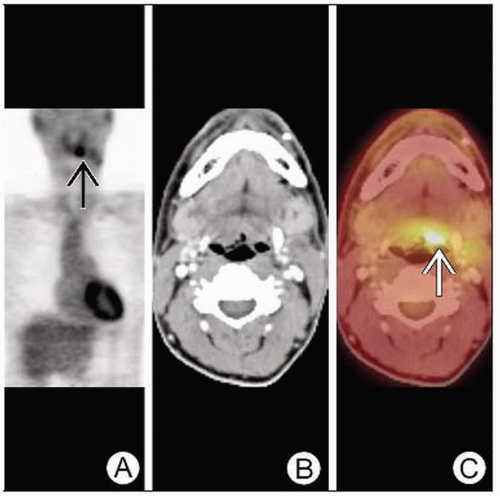 Coronal PET (A) shows focal FDG activity
 in this patient with metastatic squamous cell carcinoma but unknown primary. Axial CT (B) is normal. However, PET/CT (C) localizes the primary lesion in this patient with metastatic squamous cell carcinoma but unknown primary. Axial CT (B) is normal. However, PET/CT (C) localizes the primary lesion  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|