Elastography
Principle
Physicians have long used the technique of palpation in the clinical setting. The underlying principle of palpation lies in the ability to feel stiffer tissue in the background of softer tissue when pressed (palpated). Ultrasound brings this concept to the imaging platform wherein the deformation caused by a force can be imaged, and that deformation can be quantified either visually or quantitatively. Pathologic tissue in any organ is usually stiffer than normal healthy tissue, and thus the technology has a wide range of applications.
Imaging Based Elastography Techniques
Strain Elastography
Strain elastography (also known as real-time elastography) uses B-mode imaging as the only ultrasound technique. In this technique, the force applied over tissue is very similar to that of palpation, wherein the ultrasound operator applies force over the tissue of interest using the ultrasound transducer. This applied force causes deformation of the tissue, which can be visualized with ultrasound. Given the inherent association of operator-dependent applied nonquantifiable force, strain elastography is significantly affected by interobserver and intraobserver variability.
Shear Wave–Based Elastography
Shear wave elastography (SWE) is a technique that uses acoustic radiation force to induce microscopic tissue movements, producing tissue shear waves. Depending on whether the movement of the tissue itself is measured or whether the speed of the shear waves is measured, the technique is classified either as acoustic radiation force impulse imaging or SWE imaging. Given that the acoustic radiation force is quantifiable and constant (not observer dependent), both deformation force and tissue deformation are known in these techniques. Quantitative estimates of tissue stiffness, expressed as Young’s modulus or shear wave velocity, can be obtained.
Liver Elastography
Elastography of the liver has been predominantly used for estimation of liver fibrosis in the setting of diffuse liver disease and for the noninvasive estimation of portal hypertension.
Diffuse Liver Disease
Background and Epidemiology
The prevalence of diffuse liver disease in the United States is estimated to be as high as 14.78%. In 2010, cirrhosis secondary to diffuse liver diseases resulted in an estimated 49,500 U.S. deaths and 1.95% of all global deaths. Diffuse liver disease has several causes, including hepatic viral disease, alcoholic liver disease, nonalcoholic fatty liver disease, and autoimmune hepatitis.
Pathophysiology
Regardless of cause, chronic diffuse liver disease follows a common pathophysiologic pathway of fibrosis to severe fibrosis and eventually cirrhosis ( Figure 5-1 ). The cost of managing and treating cirrhosis is extremely high and often requires liver transplantation.

Imaging
The goal of managing diffuse liver disease is to prevent progression to cirrhosis. Therefore, reliable liver fibrosis staging is necessary to meet this goal. Unfortunately, no conventional imaging modality (i.e., ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]) has shown good sensitivity or specificity for diagnosing early or severe fibrosis. Most current imaging modalities have a high sensitivity for the diagnosis of cirrhosis, but this renders the goal of management ineffective.
Liver Biopsy
Liver biopsy currently remains the gold standard for estimation of liver fibrosis. However, liver biopsy has a number of limitations: (1) invasiveness with an estimated mortality rate of up to 0.13% and a postprocedure pain rate of up to 63.9%, (2) cost, (3) interobserver variability, and (4) sampling error (only 1/50,000th of the liver is sampled).
Hepatitis C
Epidemiology
Hepatitis C (HCV) is the most common hepatic viral disease worldwide, with an estimated prevalence of 5.2 million in the United States and more than 185 million worldwide.
Pathophysiology
HCV progresses insidiously and typically remains asymptomatic for decades, represented by the fact that that only 15% to 30% of HCV-infected patients progress to cirrhosis over a 20- to 30-year period. It has been shown that liver fibrosis of stage F2 or greater is predictive of subsequent cirrhosis in HCV-infected patients. Recent advances in therapy have been successful in curing HCV. However, these treatments are very expensive, with a per-patient drug expenditure of approximately $80,000. Treatment is therefore usually allocated to those at risk for developing cirrhosis.
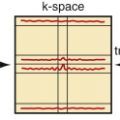
Ultrasound Elastography
Shear wave elastographic approaches have good accuracy for the diagnosis of F2 or greater liver fibrosis in patients with HCV. This technique can noninvasively distinguish varying degrees of liver fibrosis that appear identical on standard B-mode acquisition ( Figures 5-2 and 5-3 ). SWE has also shown high accuracy for the diagnosis of cirrhosis (F4 disease).


Hepatitis B
Epidemiology
An estimated 2 billion people worldwide are infected with hepatitis B (HBV). However, the majority of infected people clear the virus and only a small minority remains chronically infected. Those chronically infected can develop cirrhosis secondary to chronic liver inflammation. This at-risk population comprises over 350 million people globally.
Pathophysiology
Similar to HCV, the finding of F2 or greater fibrosis on liver biopsy carries an increased risk for subsequent cirrhosis in patients with chronic hepatitis B. Therefore, the imaging diagnosis of early fibrosis is of paramount importance.
Imaging
Similar to HCV, conventional imaging (ultrasound, CT, MRI) has no role in the diagnosis of early fibrosis in this cohort of patients. Hence, elastography is a great diagnostic imaging tool for this population.
Nonalcoholic Fatty Liver Disease
Epidemiology
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disorder, with a prevalence of 17% to 46% in the United States and a worldwide prevalence of 6% to 35%.
Pathophysiology
NAFLD can essentially be categorized in two forms: simple steatosis (~80% of cases), and (2) nonalcoholic steatohepatitis (NASH, 20% of cases), in which excess liver fat is associated with inflammation. From a clinical standpoint, it is essential to accurately distinguish the 20% with NASH at risk for cirrhosis from the 80% with simple steatosis who will not progress and require no treatment.
Imaging
Ultrasound.
Ultrasound has a modest sensitivity (67%) and specificity (77%) as a screening tool for steatosis. However, it has no role in distinguishing inflammation and fibrosis.
Computed Tomography and Magnetic Resonance Imaging.
CT and MRI can quantify liver fat, but conventional CT and MRI cannot distinguish simple steatosis and NASH, which currently requires nontargeted liver core biopsy.
Ultrasound Elastography.
In elastography, early studies have shown promise in making this differentiation. SWE has shown an area under the receiver operating characteristic curve (AUC) of 0.944 in differentiating F2 or greater fibrosis. Similarly, studies have shown AUCs of 0.90 to 0.97 in differentiating F3 or greater fibrosis.
Portal Hypertension
Cause
The hallmark of cirrhosis is portal hypertension. However, the diagnosis is best made by measuring the hepatic venous pressure gradient (HVPG).
Pathophysiology
The onset of portal hypertension after the development of cirrhosis is progressive. However, depending on severity, there is significant variation among the four stages with varying degrees of survival. The median 1-year survival in the four stages of cirrhosis has been reported to be 99%, 97%, 80%, and 43%, respectively.
Imaging
Ultrasound, Computed Tomography, and Magnetic Resonance Imaging.
Conventional imaging has high sensitivity for the detection of cirrhosis. However, there is a limited role in the diagnosis of HVPG.
Ultrasound Elastography.
Ultrasound elastography has used both liver and spleen stiffness as a direct assessment of portal hypertension. Spleen stiffness measurements can be independently used as good predictors of clinically significant portal hypertension using elastography. For diagnosing clinically significant portal hypertension, a liver stiffness value of 24.6 kPa with SWE has been reported to have a sensitivity, specificity, and accuracy of 81%, 88%, and 82%, respectively.
Contrast-Enhanced Ultrasound
Investigations of contrast-enhanced ultrasound in the abdomen are predominantly performed on liver, kidney, pancreas, and spleen for screening of anatomic structures, lesion characterization, and blood volume and perfusion evaluation.
The common enhancing patterns of focal liver lesions are well established in contrast-enhanced ultrasound ( Figure 5-4 ). The typical patterns of liver lesions include (1) contrast absence (e.g., cyst or small hemangioma); (2) diffuse hyperechoic enhancement (e.g., hepatocellular carcinoma [HCC], hypervascular metastasis, and focal nodular hyperplasia [FNH]) ( Figure 5-5 ); (3) heterogeneous enhancement (e.g., large HCC); (4) diffuse heterogeneous enhancement (e.g., HCC, lymphoma, metastasis); (5) rim-like enhancement (e.g., abscess, metastasis, cholangiocarcinoma); (6) peripheral nodular enhancement (e.g., hemangioma) ( Figure 5-6 ); (7) spoke-like enhancement (e.g., FNH); and (8) stippled heterogeneous or “basket sign” (e.g., HCC). Malignant lesions usually manifest a rapid washout, owing to arteriovenous shunts in the portal venous phase, and centripetal filling is not seen. Benign lesions usually manifest in an isoechoic homogeneous enhancing pattern. The residual central hypoechoic area is often a specific pattern for the diagnosis of FNH.