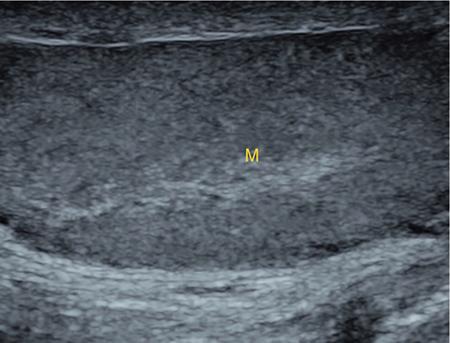
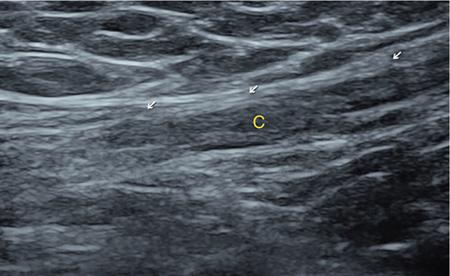
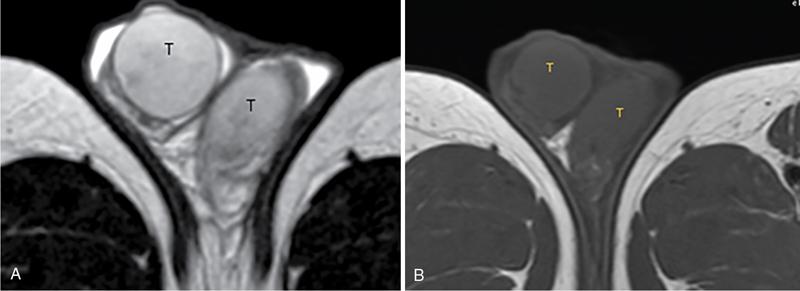
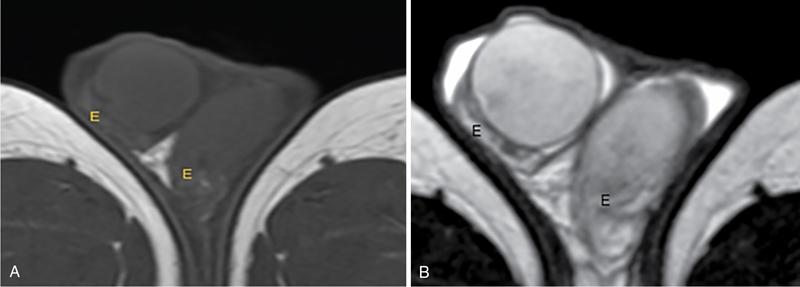
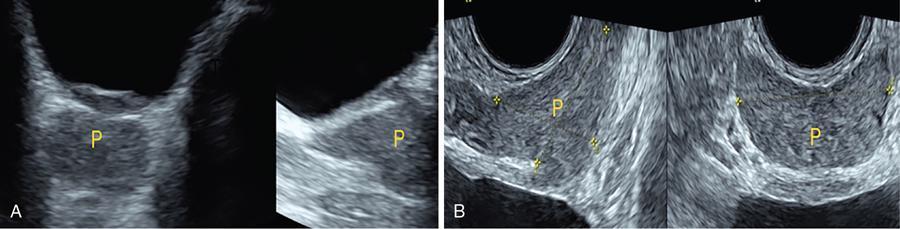
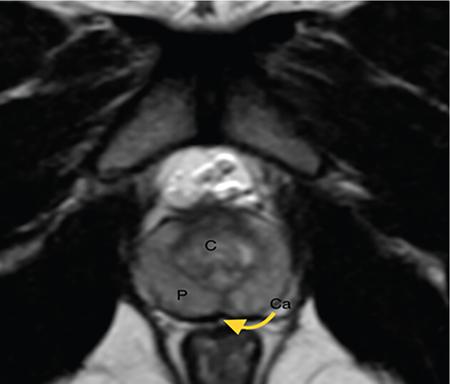
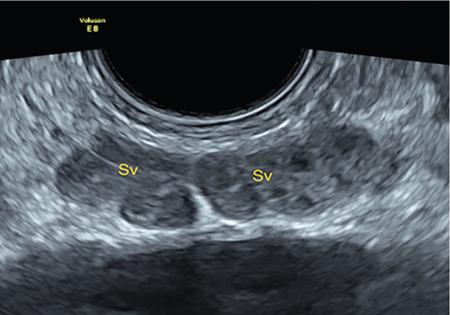
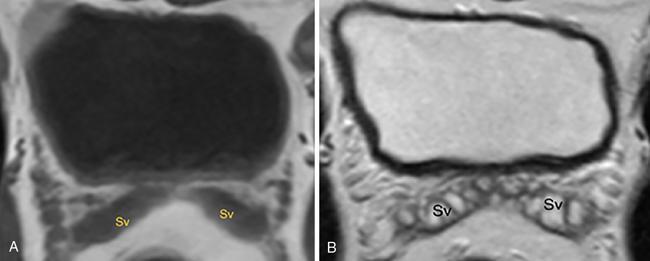
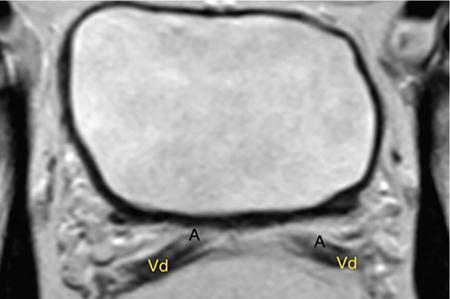
IMAGING ANATOMY OF MALE REPRODUCTIVE SYSTEM Ganesh Rajagopal The male reproductive system is formed by testes, ejaculatory ducts, seminal vesicles (SVs), prostate and penis. Various diagnostic imaging modalities like ultrasound (US), computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) are helpful in the diagnostic evaluation of male reproductive system. Various indications for imaging may include acute scrotum (testicular torsion, trauma and epididymo-orchitis), scrotal swelling (hydrocele, spermatocele, idiopathic scrotal wall oedema and scrotal abscess) and infertility. US and MRI are the commonly used imaging modalities in male reproductive system which complement each other. CT is not very useful due to poor contrast resolution. Ultrasound imaging (US) with a high-frequency linear (7.5–10 MHz) transducer probe has become the imaging modality of choice for scrotal evaluation. Scrotal US is an excellent imaging modality as it can demonstrate abnormalities in testis as well as in paratesticular structures. Scrotal wall is formed by the skin, superficial fascia, dartos muscle, the external spermatic fascia, cremasteric fascia and the internal spermatic fascia. The scrotum is divided into two cavities by a median raphe. This multilayered scrotal wall is poorly delineated in US and MRI, it is typically hypointense on both T1- and T2-weighted images. Testes are paired organs, located normally in scrotal sac, suspended by the spermatic cords. Each testis is examined in orthogonal transverse and longitudinal planes, with both grey scale and colour Doppler modes, to assess its volume and blood flow. Volume of testis is calculated by length × height × width × 0.71. A total volume (both testes) of >30 mL and a single testicular volume of 12–15 mL is generally considered normal for adults. Testes are supplied by the testicular arteries, which arise from the aorta and enter the spermatic cord at deep inguinal ring to reach the upper pole of testis. Pampiniform plexus of veins surrounds the testis and appears as a serpiginous tubular structure posterior to it, measuring >2–3 mm in diameter. Testes are oval shaped, with homogeneous echotexture on grey scale US. Along with the epididymis, they are surrounded by an echogenic capsule, known as the tunica albuginea. Tunica albuginea is covered by tunica vaginalis, which is a remnant of the processus vaginalis and both represent closed sac of peritoneum with two layers. This tunica albuginea is seen extending into posteromedial testis and form the mediastinum testis (Fig. 11.2.1.1), which consists of ducts, nerves and blood vessels. The mediastinum testis is seen as a thin echogenic band. Rete testis is formed by the convergence of seminiferous tubules, seen as a hypoechoic area adjacent to mediastinum testes. The epididymis is a comma-shaped, elongated structure placed at the posterior border of the testis, which drains the efferent ductules (Fig. 11.2.1.2). It has head, body and tail. The head overlies the superior pole of the testis and is isoechoic or slightly hyperechoic whereas, the body and tail are located behind and along the inferior pole and are usually isoechoic. The tail of the epididymis continues into vas deferens (VD), which along with the nerves, lymphatic and vascular structures, forms the spermatic cord (Fig. 11.2.1.3). The spermatic cord appears as an echogenic band in the inguinal canal. The normal adult testis is a homogeneous oval structure that appears hyperintense on T2-weighted sequences and hypointense–isointense on T1-weighted images (Fig. 11.2.1.4). The tunica which surrounds the testis is hypointense T1- and T2-weighted sequences. Epididymis is isointense on T1-weighted images but hypointense on T2-weighted images compared to testis (Fig. 11.2.1.5). Both testicles and epididymis enhance after intravenous administration of gadolinium (Gd) MR contrast agents. Prostate, though visualized by transabdominal scan is better assessed by transrectal high frequency (7.5–10 MHz) ultrasound transducer (TRUS) with patient in left lateral decubitus position. The prostate gland is divided into the anterior fibromuscular stroma (devoid of glandular tissue), transition zone, central zone, periurethral zone and peripheral zone. The base of the prostate is located superiorly and contiguous with the bladder neck whereas, the apex of the prostate is located at the inferior aspect continuous with the striated muscles of the urethral sphincter. The neurovascular bundle is seen to course near the posterolateral aspect of prostate, which is a preferential route of tumour spread. The prostate appears as a cone-shaped organ and shows uniform low echogenicity (Fig. 11.2.1.6). The outer gland (central and peripheral zones) is generally more echogenic than the inner gland. The transition and central zones of the prostate have similar MR signal intensity and cannot be differentiated, hence, are collectively referred as the central gland. On T2-weighted MR images, the normal peripheral zone is homogeneously hyperintense, whereas the central gland tissue is typically hypointense or isointense compared to the skeletal muscle (Fig. 11.2.1.7). The capsule and the anterior fibromuscular stroma appear hypointense on T2-weighted MR images. The SVs are seen as septate tubular cystic structures, appearing uniformly anechoic in US, above the prostate with distal portion of VD is seen medial to it. The duct of SV and VD joins to form the ejaculatory duct, which drains into the prostatic urethra via verumontanum. SVs show ‘bow-tie’ appearance in transversal scans, and a club or tennis-racket shape in longitudinal scans (Fig. 11.2.1.8). On MR, SVs are seen as elongated fluid-containing structures with thin septa, which is hypointense on T1 and hyperintense on T2-weighted MR images (Fig. 11.2.1.9). The VD is seen as a tubular structure with low signal intensity in both T1- and T2-weighted images, on either side. The dilated distal portion of VD (ampulla), appears hyperintense on T2-weighted images, similar to that of the SV due to the fluid content (Fig. 11.2.1.10). The penis, being a superficial organ, is usually examined with US, although MRI is reserved as problem solving modality. The penile body contains two paired muscles – corpora cavernosa and a corpus spongiosum. The former performs as a main erectile body while the latter contains the penile urethra (Fig. 11.2.1.11). Dartos fascia forms the outer layer and the Buck fascia forms the inner layer, which contain the deep dorsal vein (DDV) and a paired dorsal neurovascular bundle. The corpus spongiosum and corpora cavernosa are of high signal intensities on T2-weighted MR images and intermediate-low signals on T1-weighted MR images. The tunica albuginea being a fibrous sheath, surrounds all the three muscles, is hypointense on all sequences (Fig. 11.2.1.12). IMAGING ANATOMY OF FEMALE REPRODUCTIVE SYSTEM Saranya The female reproductive system comprises of uterus, cervix, fallopian tubes, ovaries, vagina and vulva. Ultrasonography (transabdominal and transvaginal) is the primary imaging modality of choice for imaging the female pelvis. Computed tomography (CT) is less often used for pelvic imaging. It provides a quick and systematic overview with coverage of the abdomen in the same session. Hence, CT is well suited for staging pelvic cancers and for imaging gynaecologic and nongynaecologic diseases presenting with acute abdominal pain. Pelvic anatomy is well demonstrated by magnetic resonance imaging (MRI). The contrast resolution of T2-weighted images form the basis for superb tissue characterization of MRI. Uterus is a thick-walled fibromuscular organ composed of myometrium and endometrium. It has two major divisions, namely, the body (corpus) and cervix. The fundus lies above the ostia of fallopian tubes. The normal uterus measures between 5 and 9 cm in length and is in an anteverted position, in relation to the urinary bladder. The myometrium shows three layers on USG, a compacted thin, hypoechoic inner layer forms subendometrial halo, a thicker, homogenously echogenic middle layer and a thinner, hypoechoic outer layer (peripheral to arcuate vessels). The appearance of the endometrium varies with the phase of the menstrual cycle. It appears as a thin echogenic line early in the proliferative phase and shows hypoechoic thickening (4–8 mm) as proliferative phase progresses. It shows a triple layer (sandwich or trilaminar) appearance in the mid cycle and may measure up to 12–16 mm. During secretory phase after ovulation, the layers are seen hyperechoic due to the increasing complexity of glandular structure and secretions (Fig. 11.2.2.1). Postmenopausally, the endometrium decreases in thickness. Endometrial thickness of 5 mm is taken as cut-off. Women on hormonal therapy acceptable endometrial thickness is up to 8 mm. Three-dimensional US permits multiple views to be reconstructed from a single sweep through the uterus. Sonohysterogram is the study of choice for detailed evaluation of the endometrial cavity pathologies. The cervix begins at the inferior narrowing of the uterus (isthmus) at the internal os, which is identified by the entrance of uterine vessels. It has supravaginal and vaginal portions. It is 3–4 cm long and shortens after childbirth. In premenarche women, cervix is larger than corpus, forming approximately 2/3 of the uterine mass. During menarche, there is preferential growth of the corpus and in nulliparous women, corpus and cervix are roughly equal, whereas in parous woman, corpus forms approximately 2/3 of the uterine mass. Uterus is an extraperitoneal organ. The peritoneum extends over urinary bladder dome to anterior uterus, forming anterior cul-de-sac (vesicouterine pouch) and posteriorly, the peritoneum extends more inferiorly to the upper portion of vagina, forming the posterior cul-de-sac (pouch of Douglas, rectouterine pouch), which forms the most dependent portion of the female pelvis. Supporting ligaments of the uterus comprise mainly of broad ligaments, which extend laterally to the pelvic wall and round ligaments, which arise from uterine cornu near fallopian tubes to course anteriorly, pass through the inguinal canal to insert on the labia majora. Connective tissue thickening at the base of the broad ligament forms the uterosacral ligaments posteriorly, cardinal ligaments laterally and vesicouterine ligaments anteriorly. CT examination displays the uterus as a triangular or ovoid soft tissue structure behind the urinary bladder (Fig. 11.2.2.2). Following the administration of intravenous contrast, there is enhancement of myometrium that helps to delineate the endometrium. The vagina, cervix and corpus can be differentiated by morphological characteristics and enhancement pattern. The uterine corpus is typically triangular, whereas cervix is more rounded. The vagina has an appearance of flat rectangle at the level of fornix. The broad ligament and round ligaments are seen coursing laterally and anteriorly, respectively. The main source of vascular supply to uterus is from the uterine arteries. The uterine arteries pass within the broad ligament to enter the uterus, adjacent to the lateral fornices. The uterine artery passes over the ureter at the level of the cervix. Then it courses superiorly, along the lateral margin of the uterus and anastomoses with the ovarian artery. Uterine arteries give rise to arcuate arteries, which run in the outer third of myometrium. Radial arteries extend through the myometrium, which terminate as spiral arteries in the endometrium. The venous system parallels the arterial system, forms a complex venous network in the parametrium and drains to the iliac veins. Middle and lower thirds of the uterus are drained by obturator, parametrial and paracervical lymph nodes. Lymphatic drainage from the upper corpus and fundus goes to the common iliac and paraaortic lymph nodes. MRI provides a more comprehensive view of the uterine anatomy. On MRI, the uterus and cervix show uniform low to intermediate signal on T1-weighted images. On T2-weighted images, uterus shows three distinct zones, namely high signal endometrium, low signal junctional zone and intermediate signal myometrium (Fig. 11.2.2.3). The normal thickness of the junctional zone varies from 2 to 8 mm. A thickness of 9 to 12 mm is equivocal and greater than 12 mm is abnormal. Both endometrium and junctional zone become thin with oral contraceptive intake. Endometrial atrophies and the junctional zone is absent in postmenopausal women. The endocervical canal shows high signal on T2-weighted images, whereas cervical stroma shows low signal, contiguous with the junctional zone. An outer layer of intermediate signal smooth muscle is present. Nabothian cysts representing obstructed, mucous secreting glands are commonly seen as low signal on T1-weighted images and high signal on T2-weighted images. Parametrium shows low to intermediate signal intensity on T1-weighted images and variable signal intensity on T2-weighted images. The round ligaments and uterosacral ligaments show low signal intensity, cardinal ligaments and associated venous plexuses show high signal intensity on T2-weighted images. Ovaries are located posterolateral to the body of the uterus between the uterus and the pelvic sidewall. The internal iliac vessels lie immediately posterior to the ovary. Exact position is variable due to the laxity in the ligaments, parity, uterine size and position. On USG, medulla of the ovaries is mildly hyperechoic compared to the hypoechoic cortex. Developing follicles appear anechoic (Fig. 11.2.2.4). Corpus luteum may have a thick, echogenic ring and haemorrhage is common.
11.2: Anatomy and normal variants
Introduction
Imaging anatomy of male genital system


Uterus


Ovaries
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


