Introduction
The vascular system of the human brain differs significantly, both anatomically and physiologically, from that of other organs. Although it accounts for only 2% of the body weight, the brain receives 15% of the cardiac output and consumes 20% of the body’s oxygen supply in the basal state. Unlike other arteries, the cerebral arteries are little influenced by sympathetic nervous activity, but they respond dramatically to changes in carbon dioxide and oxygen levels.
Depending on their location, obstructive lesions of the intracranial and extracranial arteries supplying the brain can cause a wide array of neurologic symptoms. The extent of clinical symptoms is strongly dependent on the presence and extent of the collateral circulation to the brain because these collaterals can help minimize the effects of arterial occlusions, decreased cerebral perfusion, and the ensuing neurologic deficit. Therefore understanding the normal and collateral anatomy of the brain circulation can help in the diagnosis of obstructive disease of the cerebrovascular system and help plan interventions.
This chapter reviews the vascular anatomy of the brain and touches on the physiologic adaptations that can help maintain cerebral perfusion and prevent permanent neurologic deficits. There is great variability in this vascular anatomy that partly explains the brain’s ability to compensate for alterations in cerebral blood flow.
As new treatment modalities become available for both extracranial and intracranial pathologies, a basic appreciation of normal anatomy, congenital variations, and collateral vascular pathways is extremely important. Endovascular treatment with angioplasty and stenting of carotid stenosis, coiling for aneurysm disease, and thrombolysis for acute intracerebral occlusions are now routinely used to treat intracranial atherosclerotic disease. Successful implementation of these interventions is helped by the knowledge of the extracranial and intracranial vascular anatomy.
Vascular Anatomy
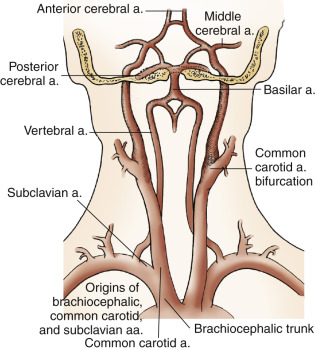
The brain is supplied directly by four vessels: the two internal carotid arteries and the two vertebral arteries. Any discussion of the cerebrovascular system begins at the origins of these vessels. The blood supply for the central nervous system derives from the three great vessels arising from the aortic arch in the superior mediastinum: the brachiocephalic (innominate), the left common carotid, and the left subclavian arteries ( Fig. 4.1 ). On the right side, the brachiocephalic trunk (innominate artery) travels upward, slightly posterior to the arch and to the right of the neck over a distance of 4 to 5 cm. It then divides into the right common carotid artery and the right subclavian artery near the right sternoclavicular junction. On the left, the common carotid and subclavian arteries have separate origins. The common carotid ascends from the arch and passes beneath the left sternoclavicular joint. Neither common carotid has collateral branches, but each divides into the internal and external carotid arteries at the level of the upper border of the thyroid cartilage.
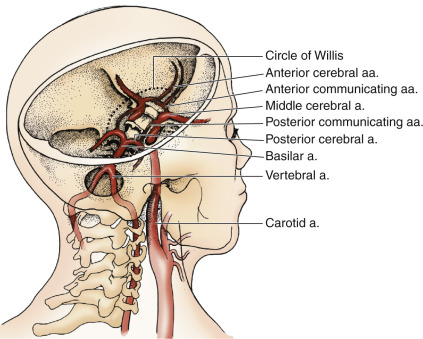
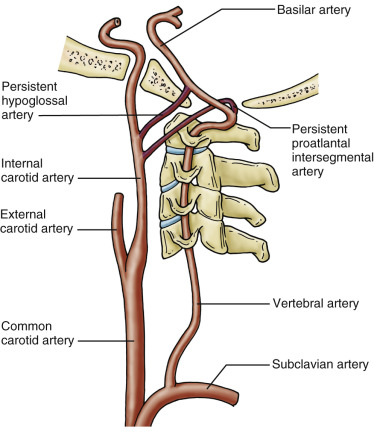
The internal carotid arteries supply most of the anterior circulation to the brain ( Fig. 4.2 ). In its cervical portion, the internal carotid artery may be relatively straight or may have a tortuous course as it travels to the base of the skull. With the exception of very rare anomalies, there are no branches of the internal carotid artery in the neck. Specific exceptions include cases where the embryonic connections between the vertebral and cervical carotid systems fail to involute and cases of aberrant origin of some external carotid artery branches from the proximal internal carotid artery. The persistent hypoglossal artery communicates between the basilar artery and the cervical internal carotid artery and the persistent proatlantal intersegmental artery that communicates between the vertebral artery and the internal carotid, at a location lower than the persistent hypoglossal would have connected ( Fig. 4.3 ). The most common cases of aberrant origin branches from the internal carotid artery are the ascending pharyngeal (1.7% to 6.2%), the occipital (0.2% to 0.49%), and very rarely the (internal) maxillary arteries. As the internal carotid proceeds through the carotid canal in the temporal bone, the internal carotid artery gives rise to the caroticotympanic branches in the petrous bone, the meningohypophyseal branches in the cavernous sinus region, multiple branches within the cavernous sinus, and the ophthalmic arteries immediately distal to the cavernous sinus. The internal carotid artery shares the carotid canal with the sympathetic nervous plexus. Eight millimeters beyond the clinoid process, within the dura mater, the internal carotid artery gives rise to the posterior communicating arteries, which join the posterior cerebral arteries. More cephalad, the internal carotid artery divides into the middle and anterior cerebral arteries and gives rise posteriorly to the anterior choroidal arteries.
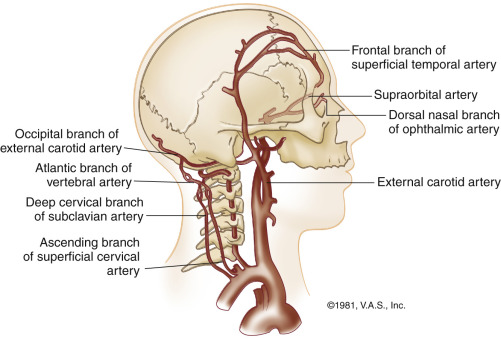
The external carotid artery normally does not supply blood flow to the brain. However, several of its branches can become important collateral pathways if the internal carotid or vertebral arteries become occluded. The branches of the external carotid artery are the superior thyroid, the ascending pharyngeal, the occipital, the lingual, the facial, the (internal) maxillary, the posterior auricular, and the superficial temporal arteries. The external carotid artery branches more often develop as collaterals to the ophthalmic artery in case of occlusive lesions of the internal carotid artery and to the muscular branches of the occipital and vertebral arteries in cases of proximal vertebral artery occlusions ( Fig. 4.4 ).
The posterior circulation to the brain is supplied mainly by the vertebral arteries. The vertebral arteries arise from the subclavian arteries except for the left vertebral artery that can have a direct origin from the aorta in 3% to 5% of patients. The proximal vertebral artery (V1) enters the foramen transversarium at C 6 and continues to lie within it (V2) until C 2 , and then winds anteriorly to the subarachnoid space at the side of the medulla oblongata at the level of the atlantooccipital interspace (V3). Having entered the dura, it proceeds upward and anteriorly (V4), giving off the posterior inferior cerebellar arteries, then reaching the pontomedullary level where it joins the contralateral vertebral artery to form the basilar artery. Four branches arise from the basilar artery as it courses upward before dividing into the posterior cerebral arteries. Branches of the basilar artery supply the entire pons and the superior and anterior aspects of the cerebellum. Branches of the vertebral arteries supply the medulla and the interior surface of the cerebellum.
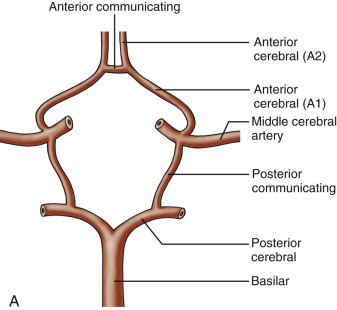
The intracranial branches of the internal carotid and vertebral arteries are joined at the base of the brain by an arterial circle known as the circle of Willis. This is the critical component of the intracranial collateral circulation and is also a common site of aneurysm formation. It is a hexagonal arrangement of arteries composed of the anterior, middle, and posterior cerebral arteries, which are joined together by the anterior and posterior communicating arteries ( Fig. 4.5A ). Under normal circumstances, there is little mixing of blood through the communicating arteries. However, in instances of arterial occlusion of the carotid or vertebral-basilar arteries, the different branches in the circle can open and serve as collateral pathways.

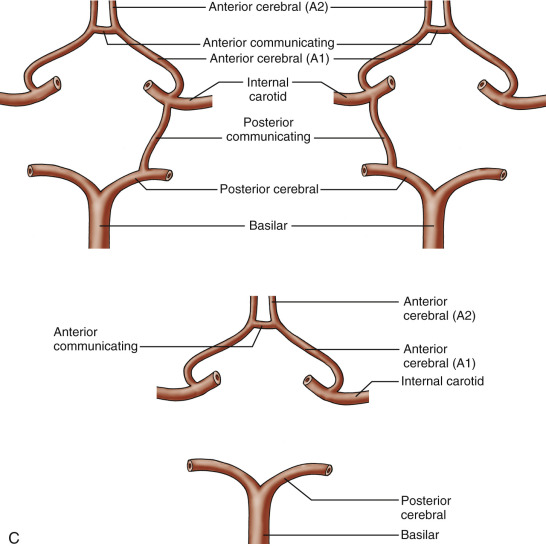
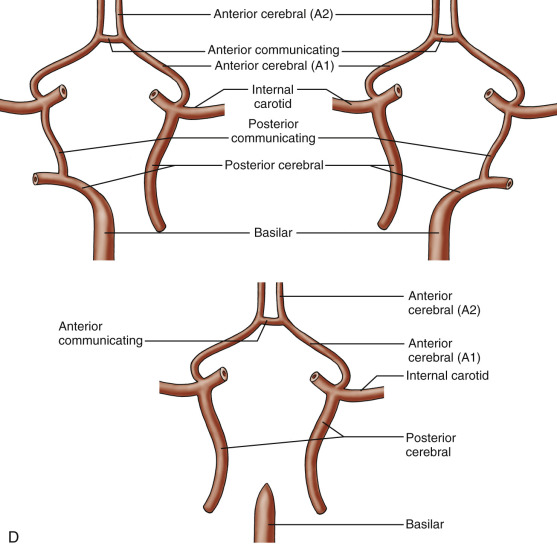
Component arteries of the circle of Willis can vary greatly in size (see Fig. 4.5B ), and there are many congenital variations in the structure of the circle, with the major ones as shown (see Fig. 4.5C and 4.5D ). The most common anomalies involve the absence or hypoplasia of one or both communicating arteries (see Fig. 4.5C ). An anomalous origin of the posterior cerebral artery from one or both internal carotid arteries has also been commonly encountered (see Figs. 4.5D ). Anomalies in the anterior portion of the circle are uncommon and most often consist of duplications. Absence or hypoplasia of the proximal segment of the anterior cerebral artery between the internal carotid and anterior communicating arteries is rare. The most important variants are those that decrease pathways for possible collateral flow and occur when the anterior or posterior communicating arteries are absent or atretic. These conditions may isolate the anterior and posterior circulations or the left and right hemispheric carotid territories.
The typical branching pattern of the aortic arch is shown in Fig. 4.6A . Congenital variations in the extracranial arteries are commonly seen at the origins of the carotid and vertebral arteries from the aortic arch. The most frequent congenital variation is a sharing or close association between the origin of the brachiocephalic artery with the left common carotid artery, also called bovine arch, with two variants: less often (5% to 7%), the left common carotid artery may arise from the brachiocephalic artery (see Fig. 4.6B ), or have a shared origin with the brachiocephalic artery with a prevalence of approximately 20% (see Fig. 4.6C ). An anomalous origin of the left vertebral artery from the aortic arch between the left common carotid and subclavian arteries has a low prevalence of 3% to 5% (see Fig. 4.6D ). Rarely, the right subclavian artery may have an aberrant origin from the aortic arch distal to the left subclavian artery. Other abnormalities can occur in the cervical region, such as agenesis of the internal carotid arteries, but these are rare. Besides a direct origin of the left vertebral artery from the arch, abnormalities in the vertebral arteries are usually limited to variations in size between the left and right, referred to as vertebral artery dominance. The left tends to be more dominant in about 40% of patients, the right in about 30%, and both are equal in the remaining.
Related posts:
 Anatomy of the Upper and Lower Extremity Arteries
Anatomy of the Upper and Lower Extremity Arteries
 Ultrasound Assessment Following Endovascular Aortic Aneurysm Repair
Ultrasound Assessment Following Endovascular Aortic Aneurysm Repair
 Ultrasound Assessment of Carotid Stenosis
Ultrasound Assessment of Carotid Stenosis
 Assessment of Upper Extremity Arterial Disease
Assessment of Upper Extremity Arterial Disease
 Ultrasound Assessment Following Endovascular Aortic Aneurysm Repair
Ultrasound Assessment Following Endovascular Aortic Aneurysm Repair
 Evaluation of Organ Transplants
Evaluation of Organ Transplants
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


