Fig. 2.1
Anatomy of the pancreas. Diagram illustrates the complete anatomic components of the pancreas
Fig. 2.2
Pancreas position. Illustration (a), 3D volume-rendered reconstruction coronal and axial planes (b, c) display the oblique position of the pancreas in the retroperitoneum
Fig. 2.3
Pancreas shape. Diagram (a), transverse scan of the pancreas on conventional ultrasound (b), contrast-enhanced CT axial image (c), and contrast-enhanced magnetic resonance axial image (d) show the shape of the pancreas similar to the letter J turned sideways with the loop of the J around the duodenum
The pancreas is a large accessory digestive gland.
Covered with fine connective tissue but does not have a true capsule.
Situated in the retroperitoneum in the anterior pararenal space.
Lies in an oblique position posterior to the stomach.
Extends across the abdomen, from the concavity of the duodenum to the splenic hilum at the level of T12/L1–L3 (Fig. 2.2).
The pancreas is bordered by the lesser sac above, the transverse colon anteriorly, and the peritoneal cavity below.
The shape of the pancreas is compared to the letter “J” turned sideways with the loop of the “J” around the duodenal C-loop (Fig. 2.3 ).
The average adult pancreas weighs 60–120 g and measures 15–20 cm in length.
The pancreas’ dimensions vary from patient to patient depending on the patient’s age and habitus.
Practical Pearls
Absolute measurements of the pancreas are controversial therefore, measurements taken by imaging are not recommended for diagnosing pancreatic enlargement.
The most important parameters by imaging to determine a pancreatic abnormality are (a) focal or diffuse enlargement; (b) contour irregularity; (c) abnormal echogenicity, density, or intensity of the pancreatic parenchyma; (d) abnormal echogenicity, density, or signal intensity of the peripancreatic fat; and (e) dilatation of the pancreatic or common bile ducts, or both.
2.2.1 Pancreatic Divisions and Anatomic Relationships (Figs. 2.4–2.6)
Fig. 2.4
Divisions of the pancreas. Illustration (a), gross specimen of cadaveric pancreas (b), and 3D volume-rendered reconstruction coronal (c) and axial (d) show the divisions of the pancreas. H head, UP uncinate process [(a, b) (curved arrows), (c, d) (arrows)], N neck, B body, T tail
Fig. 2.5
Anatomic relationship of the pancreas (P) with surrounding organs and structures on computed tomography, axial plane. 3D volume-rendered axial reconstruction displays the 1 splenic vein, 2 spleen, 3 left kidney, 4 left adrenal gland, 5 superior mesenteric vein, 6 superior mesenteric artery, 7 aorta, 8 right renal artery, 9 inferior vena cava, 10 right kidney, 11 ascending colon, 12 common bile duct, 13 junction of superior mesenteric vein and splenic vein, 14 gallbladder, 15 duodenum, 16 left lobe of the liver, 17 antrum of the stomach, 18 lesser sac, and 19 body of the stomach
Fig. 2.6
Anatomic relationship of the pancreas (P) with other surrounding organs and structures on computed tomography, coronal plane. 3D volume-rendered coronal reconstruction displays the 1 splenic vein, 2 left kidney, 3 superior mesenteric vein, 4 superior mesenteric artery, 5 aorta, 6 junction of the superior mesenteric vein with splenic vein, 7 right kidney, 8 duodenum, 9 liver, 10 gallbladder, 11 splenic artery, 12 stomach, and 13 spleen
Head
Widest portion of the gland; cupped by C-shaped curve of the duodenum.
The inferior vena cava, the right renal artery, and both renal veins lie posterior to the head of the pancreas.
Uncinate process
Inferomedial extension (prolongation) of the head of the pancreas.
Has a triangular or wedge shape.
Lies between the superior mesenteric vessels and the aorta.
Size of the uncinate process varies.
Neck
Arbitrary junction between the head and body of the pancreas
Lies directly over the junction of the splenic vein and superior mesenteric vein
Body
Runs obliquely upward to the left of the superior mesenteric vessels
Located posterior to the lesser sac and anterior to the aorta, left adrenal gland, left kidney, and renal vessels
Tail
Located close to the splenic hilum without a discernible junction point with the body.
Situated to median to the colonic flexure and anterior to the left kidney.
The most distal portion of the tail of the pancreas passes between the peritoneal layers of the splenorenal ligament along the splenic artery and the beginning of the splenic vein (intraperitoneal portion).
2.2.2 Pancreatic and Biliary Duct System
2.2.2.1 Main Pancreatic Duct (PD) (Wirsung) (Fig. 2.7)
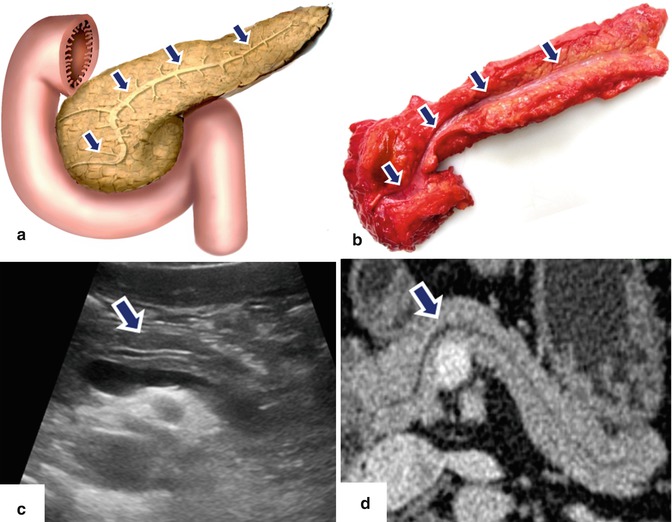
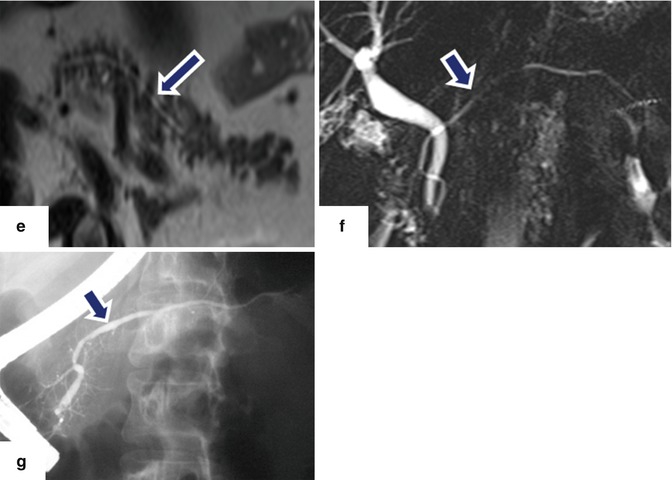
Fig. 2.7
Main pancreatic duct (Wirsung) (PD). Illustration (a), gross specimen of a cadaveric pancreas (b), conventional ultrasound transverse scan (c), contrast-enhanced CT (d), T2-weighted axial magnetic resonance image (e), MRCP (f), and ERCP (g) show the main pancreatic duct and side branches (arrows)
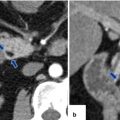
Fig. 2.8
Location of the major papilla. Illustration (a), contrast-enhanced CT coronal plane (b), and MRCP (c) images show the position of the major papilla (arrows) in the second portion of the duodenum (arrows) Illustration (d) and, contrast-enhanced CT coronal plane (e), and MRCP (f) images show the position of the major papilla (arrows) in the third portion of the duodenum (arrow)
The main pancreatic duct (Wirsung) starts in the tail and extends transversally into the head of the pancreas where it turns downwardly and posteriorly.
The main pancreatic duct receives 20–35 tributaries along its course.
The normal diameter of the pancreatic duct:
Head: 3–4 mm
Body: 2–3 mm
Tail: 1–2 mm
The diameter of the main pancreatic duct increases with age and pancreatic disease.
2.2.2.2 Accessory Pancreatic Duct (Santorini) (Figs. 2.9)
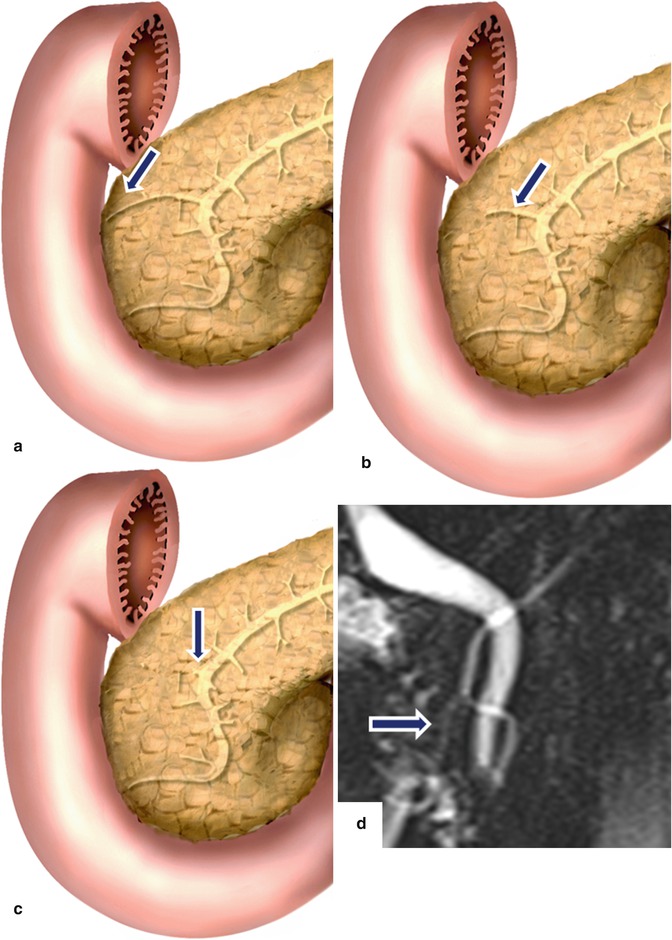
Fig. 2.9
Accessory pancreatic duct (Santorini) variants. Illustrations demonstrate the accessory duct draining into the minor papilla (a) (arrow) ending blindly (b) (arrow) and (c) show the absence of the accessory duct (arrow). MRCP shows the accessory duct ending in the minor papilla (d) (arrow)
The accessory pancreatic duct (Santorini) drains a small portion of the upper anterior aspect of the head of the pancreas.
It drains into the minor papilla, 2 cm superomedial to the major duodenal papilla.
This duct ends as a blind accessory duct in 30 % of the patients or may be completely absent.
Practical Pearls
The largest diameter of the pancreatic duct is in the head and it tapers toward the tail.
Focal dilatation of the pancreatic duct may be an early sign of a pancreatic malignancy and should be further investigated.
Most of the time, the Santorini duct is not identified by computed tomography or magnetic resonance.
A prominent accessory duct raises the possibility of a pancreatic divisum.
2.2.2.3 Common Bile Duct (CBD) (Figs. 2.10–2.12)
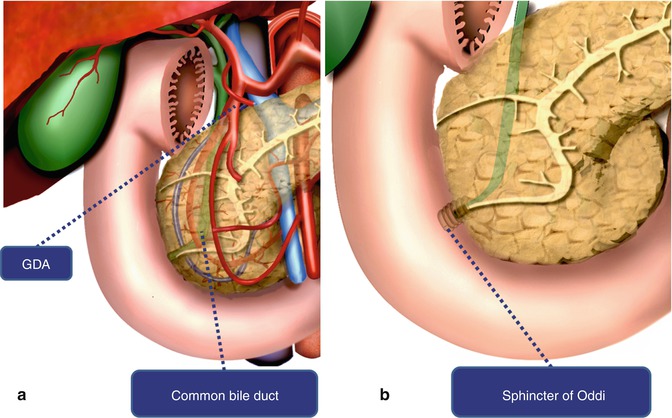
Fig. 2.10
Common bile duct (CBD). Diagram shows the relation of the common bile duct with the gastroduodenal artery (GDA) (a) and its termination in the major papilla (Sphincter of Oddi) (b)
Fig. 2.11




Variations in the junction of the common bile and pancreatic duct in major ampulla. Illustrations and MRCP thick slab images show a short common channel (a) (arrows), a long channel (b) (arrows) and no common channel between the CBD and PD at the apex of the pailla (c) (arrows)
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
