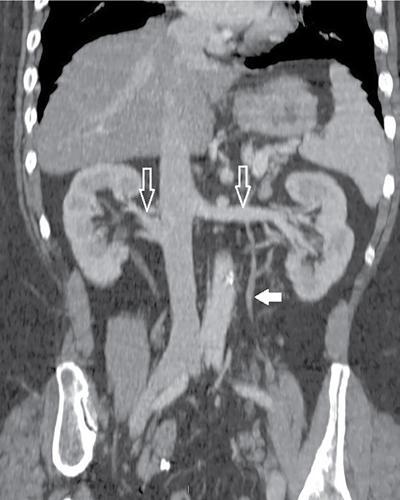
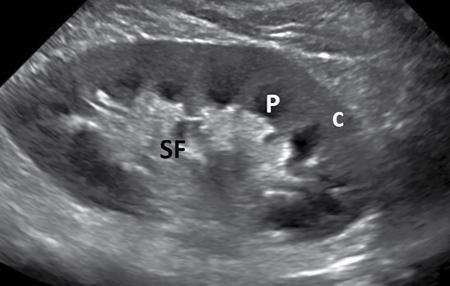
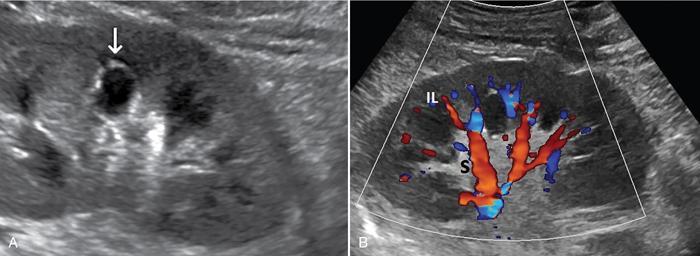
Amit Kumar Kamble, Abhinav Ranwaka The adult urinary system is formed of a pair of kidneys, a pair of ureters, a urinary bladder and a urethra. All these structures are extraperitoneal in location and extend from upper abdomen to the pelvis and into the exterior. These organs can be visualised on a host of imaging modalities, and a knowledge of these appearances helps the radiologist identify the relevant pathologies. Having a complex embryological development, the urinary system can have a wide spectrum of normal and abnormal anatomical variants. This chapter describes the appearance of the urinary system in commonly used imaging modalities and their common variants. Kidneys are paired bean-shaped structures situated in the retroperitoneum on either side of the vertebral column. The kidney consists of The renal sinus contains: The kidneys are surrounded by the renal capsule which is enclosed in the perirenal space. This space predominantly contains the perinephric fat and has thin septations within (Kunin’s septa); these septae may be thickened in various renal pathologies seen as perinephric stranding on imaging. The perirenal space is bounded by the perirenal fasciae, called the Gerota fascia (anterior perirenal fascia) and Zuckerkandl fascia (posterior perirenal fascia). The leaves of perirenal fascia fuse superiorly, laterally and medially. Superiorly, the perirenal fasciae also enclose the adrenal gland, which is separated from the kidney by a septum (Fig. 10.2.2). The anterior and posterior perirenal fasciae fuse laterally to form the lateral conal fascia. Medially, the perirenal fascia also encloses the renal pedicle. Medially, it communicates with renal sinus fat. There may be the communication of perirenal spaces across the midline. Superiorly, the perirenal space communicates with the bare area of the liver or spleen. The ureter arises from the perirenal space and travels inferiorly in anterior pararenal space. Inferiorly, the perinephric space may communicate with periureteric tissues. Interfascial planes are potential planes in between the leaves of the anterior perirenal fascia, called the retromesenteric plane and in the anterior perirenal fascia called the retrorenal plane. Anterior pararenal space: It is bounded by parietal peritoneum anteriorly, anterior perirenal fascia (Gerota) posteriorly and lateral conal fascia laterally. The anterior pararenal space contains the pancreas, second and third part of the duodenum, the retroperitoneal segments of ascending and descending colon and the roots of the small bowel mesentery and transverse mesocolon. Posterior pararenal space: It is bounded by posterior perirenal fascia (Zuckerkandl) anteriorly, fascia transversalis posteriorly and lateral conal fascia laterally. Caudally, the pararenal spaces communicate with each other and also with the extraperitoneal spaces. All the three spaces communicate at the pelvic brim. Understanding of the anatomy of spaces around the kidney is important for local staging of renal pathologies. Renal arteries are the branches of abdominal aorta. They originate laterally from the aorta below the origin of superior mesenteric artery. Accessory unilateral renal artery occurs in 30% of the population and bilaterally in 10% of population. Renal artery is divided into anterior division, which divides into four segmental branches and a posterior division; these arteries are end arteries supplying the respective segments of the kidneys (Fig. 10.2.3): apical, upper, middle, lower segments supplied by the anterior division, and a posterior segment supplied by the posterior division. The segmental arteries divide into lobar branches one to each to renal pyramid. Before reaching to pyramid, they divide into two to three interlobar branches. At the junction of cortex and medulla, interlobar arteries divide into arcuate arteries at the right angle. They further subdivide into interlobular artery, afferent and efferent arterioles. The efferent arteriole drains into peritubular plexus. The plane where the branches of the anterior and posterior divisions meet is located between the anterior two-thirds and posterior one-third of the kidney and is relatively avascular; it is called the avascular plane of Brodel (Fig. 10.2.3), and is a relatively safe site for nephrostomy access. Peritubular plexus converges to form the interlobular vein. These veins accompany their arterial counterparts and drain into the renal vein. The renal veins are situated anteriorly to the renal arteries and finally drain into the inferior vena cava at the right angles (Fig. 10.2.4). The two left renal veins may be present one passing anterior and other posterior to the aorta known as persistence of renal collar. Sometimes a single retroaortic left renal vein (Fig. 10.2.5) may be present. Supernumerary right renal vein may be seen. Renal vein variations are more common on the right side. The lymphatics of the kidneys drain into the lateral aortic nodes at the level of origin of renal arteries. Normal kidneys may be visualised on a frontal abdominal radiograph as faint oval shadows on either side of the vertebral column immediately besides the psoas shadows (Fig. 10.2.6). On contrast radiography and intravenous urography, the renal shadows show gradual opacification, peaking between 30 and 60 seconds followed by opacification of the pelvicalyceal system on subsequent radiographs. The kidneys are visualised in longitudinal and transverse views usually by placing the probe in the loin with the patient in supine or lateral position. The normal kidneys appear less echogenic than the liver and show a thin echogenic capsule. The surface of the kidney is usually smooth in adults, and may be lobulated in infants and young children. The renal parenchyma shows an outer cortex, which generally shows a uniform thickness, surrounding the less echogenic medullary pyramids, with invaginations of the columns of Bertin between the medullary pyramids (Fig. 10.2.7). This differentiation between the echogenicity of the cortex and medulla is called corticomedullary differentiation, which is lost in certain disease states. The renal pyramids are most hypoechoic compared in infancy gradually becoming less hypoechoic with age. The hypoechoic renal pyramids may at times be confused for hydronephrosis by an inexperienced observer. Arcuate arteries may be identified in some adults between the cortex and medulla as linear echogenic lines (Fig. 10.2.8A) and should not be mistaken for calculi. The renal sinus is seen as a central hyperechoic area of the kidneys owing to the presence of fat. The renal calyces and pelvis are not visualised normally as they are collapsed. They may sometimes be seen if the bladder is overdistended, a finding which reverses once the patient emptied the bladder. Doppler interrogation allows evaluation of the renal vasculature in great detail. The renal artery, its segmental, interlobular and arcuate branches and the corresponding veins can be easily visualised (Fig. 10.2.8B). At the renal hilum, the renal vein lies anterior to the renal artery. The right renal artery is longer and lies posterior to the inferior vena cava (IVC). The left renal vein crosses midline and courses in between the aorta and superior mesenteric artery. On CT scan (Fig. 10.2.9), the kidneys are well identified and well demarcated owing to the presence of surrounding fat. They show a homogeneous appearance with intermediate density between 35 and 55 HU on non-contrast CT scan with a central low-density renal sinus.
10.2: Anatomy, radiological anatomy, normal variants
Introduction
Kidney
Anatomy
Relations
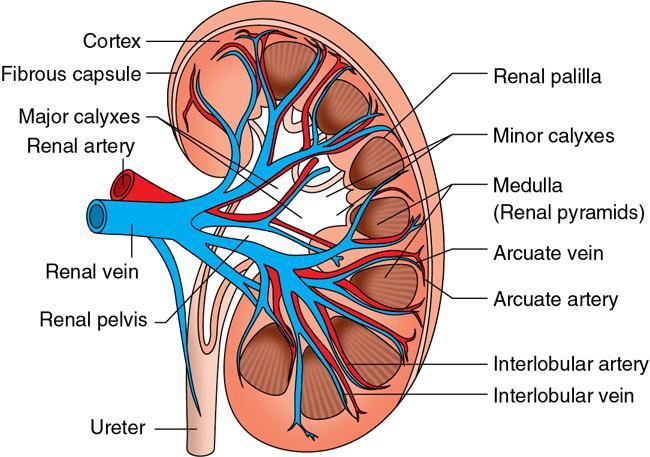
Internal structure (Fig. 10.2.1)
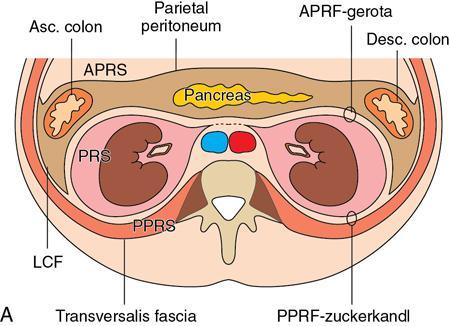
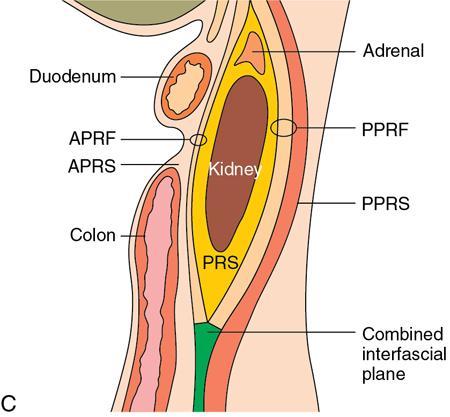
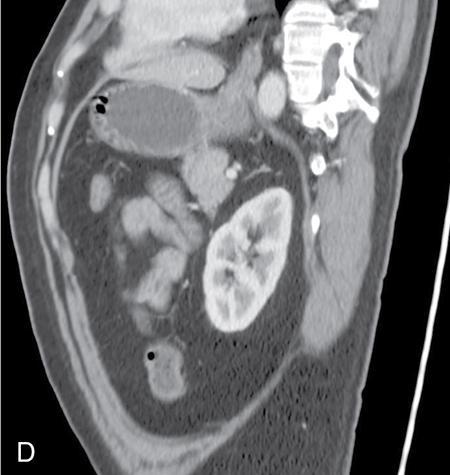
Spaces around the kidney (Fig. 10.2.2)
Perirenal (perinephric) space.

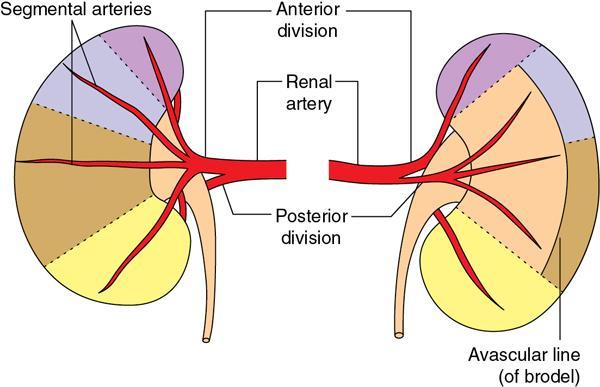
Arterial supply
Venous drainage

Lymphatic drainage
Imaging anatomy
Conventional radiology

Ultrasonography
CT scan

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


