KEY POINTS
A wide variety of congenital anomalies can affect the cerebellum. The antenatal findings overlap among different pathologies and normal variants. Consequently, a specific diagnosis is often not possible.
One of the most common abnormal findings that is encountered is the impression of a communication between the fourth ventricle and the posterior cisterna magna. When this is seen after 20 postmenstrual weeks’ gestation, it identifies a group of conditions that are commonly referred to as the Dandy-Walker complex.
Within the Dandy-Walker complex, cases with a normal appearance of the vermis and cisterna magna most frequently have a normal outcome. Fetuses with an enlarged cisterna magna and/or an abnormal vermis frequently exhibit abnormal development, but a precise prognosis is difficult to predict.
A large cisterna magna (> 10 mm) when isolated, usually has a good outcome.
Other cerebellar anomalies can be encountered, but the diagnosis is often difficult or impossible and the prognosis difficult to predict.
Abnormal sonographic findings of the posterior fossa are among the most common reasons for referral in tertiary care centers for fetal neuroimaging. They represent a major diagnostic challenge, and inaccurate interpretation with significant implications for counseling and management has been reported.1,2 The problem is two fold: On the one hand, sonography is not an ideal tool for the visualization of the posterior fossa structures, particularly in the second trimester of gestation; on the other hand, many different entities, ranging from normal variants to severe anomalies, may have a similar sonographic appearance.1,2,3,4,5 Categorization of these entities is still controversial, and there is no uniform approach.2,6,7 In this chapter, we report our own vision of the problem and our own approach, which is summarized in Table 8–1.4
| Diagnosis | TCD | Vermis Biometry | Superior/Inferior Ratio | Fastigium | Fourth Ventricle | Pons | Prognosis |
|---|---|---|---|---|---|---|---|
| Delayed “closure” | N | N | N | N | Open | N | Good |
| Vermian hypoplasia | N | Small | N | N | Open/closed | N | Variable |
| Vermian agenesis | N/S | Small | Abnormal | Abnormal | Abnormal | N | Malformations |
| Dandy-Walker malformation | N | –/Small | Abnormal | Abnormal | Abnormal | N | Poor |
| Joubert and related syndromes | N/S | –/Small | Abnormal | Abnormal | Abnormal | ? | Poor |
| Pontocerebellar hypoplasia | S | S | N | No | Normal | Abnormal | Poor |
| Rhombencephalosynapsis | S | – | – | Abnormal | Abnormal | N | Poor |
We stress that many difficulties are encountered in assessing antenatally this area of the brain and that frequently an accurate diagnosis cannot be made in utero.
Dandy-Walker malformation, vermian agenesis, vermian hypoplasia, Blake’s pouch cyst
Megacisterna magna, Joubert and related cerebellar syndromes (vermian agenesis/hypoplasia with “molar tooth” sign)
The term Dandy-Walker syndrome, subsequently modified to Dandy-Walker malformation, was originally introduced to indicate the association of (1) ventriculomegaly of variable degree, (2) a large cisterna magna with elevation of the tentorium, and (3) a defect in the cerebellar vermis through which the cyst communicates with the fourth ventricle.8 The term Dandy-Walker complex (or continuum) was later introduced to indicate a spectrum of anomalies that also include other conditions with anatomical similarities to the classic description of Dandy-Walker malformation.3,6 At present, the categorization of posterior fossa anomalies remains controversial, and there is no general consensus. We will include in this section three entities that share in common one sonographic finding: the impression that in an axial plane of the head the fourth ventricle is open posteriorly and communicates with the cisterna magna. In the following we will refer to this finding as the “open fourth ventricle.” The anomalies that demonstrate this sign are heterogeneous and include the Blake’s pouch cyst, vermian agenesis/hypoplasia, and Dandy-Walker malformation.4 The rationale for grouping them together is that they are often difficult to differentiate, and they overlap clinically.
Dandy-Walker malformation has an estimated prevalence of about 1 in 30,000 births and is found in 4% to 12% of all cases of infantile hydrocephaly.9 The incidence of the other varieties of the Dandy-Walker complex is unknown.
Different theories have been proposed. The element in common to the Dandy-Walker complex is an expansion of the fourth ventricle that displaces superiorly the cerebellar vermis. Prior to midgestation, the fourth ventricle is large, and the cerebellum does not cover it entirely. Only after 20 weeks does the cerebellum completely enfold the fourth ventricle. Many cases of the mildest anomaly in this group, the Blake’s pouch cyst, resolve spontaneously throughout gestation and therefore probably represent a delay in normal anatomical development. In other cases, the expansion of the fourth ventricle is concomitant with aberrant development of the cerebellum, and of the vermis in particular, and these cases are more likely to be associated with neurologic compromise. The Dandy-Walker malformation was originally described in individuals with obstructive hydrocephaly and was postulated to arise from a primary atresia of the foramina of Luschka and Magendie.8,9,10 A similar explanation was proposed for the Blake’s pouch cyst.11 It is now clear that most patients with the Dandy-Walker complex do not develop hydrocephaly, suggesting that the pathogenesis is more complex and is not merely the consequence of obstruction and overdistention of the fourth ventricle.3,4,6,12,13 Several hypotheses have been formulated, but there is no clear evidence supporting any of them.
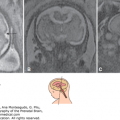
Blake described a normal embryological remain, a fingerlike outpouch of the fourth ventricle, that is commonly found below the cerebellar vermis. This structure is now referred to as the Blake’s pouch and can be sonographically demonstrated in most fetuses, particularly during the early second trimester.14 Enlargement of the Blake’s pouch (or of the entire fourth ventricle in the most severe forms) is responsible for the superior displacement of the vermis that is encountered in the Dandy-Walker complex. The enlarged Blake’s pouch/fourth ventricle balloons into the cisterna magna and in the most severe cases obliterates it and distends the posterior fossa. With most techniques of diagnostic imaging, whether prenatal or postnatal, the thin walls of the Blake’s pouch/fourth ventricle are difficult to visualize, and the impression is that of a communication between the fourth ventricle and the cisterna magna (Figure 8–1).
Figure 8–1.
The open fourth ventricle sign. (A) A sagittal view demonstrates the slight superior rotation of the cerebellar vermis that results in the presence of a fluid between the brainstem and the inferior surface of the vermis (arrow). (B) A low axial section in the same case as A. The presence of fluid between the cerebellar hemispheres suggests communication between the fourth ventricle (4v) and the posterior cisterna magna (arrow). (C) In a slightly higher section, the vermis is seen closing the fourth ventricle posteriorly.

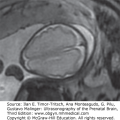
In this chapter, the term Blake’s pouch cyst is reserved for cases in which the cisterna magna is not enlarged, and the cerebellar vermis is intact. Typically in these cases, the superior displacement is mild (Figure 8–2).4,6,12,13
Figure 8–2.
Blake’s pouch cyst. (A) Pathologic specimen of a fetus at 20 weeks. An intact cerebellar vermis is slightly displaced superiorly; the thin walls of the Blake’s pouch have been disrupted in the preparation of the specimen. (B, C) Magnetic resonance imaging (MRI) of a neonate; slight superior displacement of the vermis with the open fourth ventricle (4v) sign in the axial plane (arrow). (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

Vermian agenesis/hypoplasia is characterized by a small vermis (Figure 8–3); the term hypoplasia should be reserved for cases in which the vermis is small but has a normal appearance (all the lobules are present); the term partial agenesis should indicate those cases in which a part, typically the most inferior portion, is absent. In these patients, the cisterna magna has a normal size. This condition was originally defined as Dandy-Walker variant, a term no longer in use.7,15,16
Figure 8–3.
Vermian hypoplasia. (A, B) Pathologic specimens of two affected fetuses at midgestation. In both cases, the vermis (arrow) is superiorly displaced and appears small and rudimentary with no evidence of lobulation. There is a prominent aditus to the fourth ventricle (4v). As in the previous figures, the thin walls of the Blake’s pouch have been disrupted in the preparation of the specimen. (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

Dandy-Walker malformation is characterized by the enlargement of the cisterna magna, with elevation of the tentorium and torcular herophili. The cerebellar vermis may be intact or incompletely formed but is usually significantly displaced upward (Figure 8–4). Hydrocephaly was classically considered an essential diagnostic element of this condition, but more recent evidence suggests that it is not present at birth in most patients, although it may develop in later life.8,9
Figure 8–4.
Dandy-Walker malformation. (A) Pathologic specimen from a midtrimester fetus. (B, C) MRI of an affected infant. There is a major displacement of the vermis that forms a right angle to the brain stem and the cisterna magna is enlarged; the tentorium cerebellii and the torcular herophili (TH) are displaced cranially as well. The fourth ventricle (4v) appears open. (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

Genetic factors have a major role in the etiology of the Dandy-Walker complex. Dandy-Walker malformation and vermian hypoplasia/agenesis may occur as a part of mendelian disorders and chromosomal aberrations.17 In rare cases, the disease is inherited as an autosomal recessive or dominant trait. Environmental factors, including viral infections, alcohol abuse, and diabetes, have also been suggested as playing a role in the genesis of Dandy-Walker malformation, but the evidence is uncertain.17
In the absence of a recognizable syndrome, a recurrence risk of 1% to 5% is suggested for Dandy-Walker malformation and vermian hypoplasia/agenesis.17 Autosomal transmission, both dominant and recessive, has been documented. There is no available information on Blake’s pouch cyst.
The Dandy-Walker complex (particularly Dandy Walker malformation and vermian hypoplasia/agenesis) is frequently associated with chromosomal aberrations, syndromes and other cerebral malformations (mostly ventriculomegaly, agenesis of the corpus callosum, holoprosencephaly, and cephaloceles), polycystic kidneys, cardiovascular defects, and facial clefting.15,18,19 Postnatal studies of infants with the classic type of Dandy-Walker malformation indicate a frequency of associated malformation ranging from 50% to 70%.8,9,10 A detailed list of conditions found in association with Dandy-Walker malformation is given in Table 8–2.
| Mendelian | Environmental |
|---|---|
| Warburg (AR) | Rubella |
| Aase-Smith (AD) | Coumadin |
| Ruvalcaba syndrome (AD/X-linked) | Alcohol |
| Coffin-Siris (AR) | Cytomegalovirus |
| Orofaciodigital syndrome type II (AR) | Diabetes |
| Meckel-Gruber syndrome (AR) | Isotretinoin |
| Aicardi syndrome (X-linked dominant) | Multifactorial |
| Ellis-Van Creveld (AR) | Congenital heart disease |
| Fraser cryptophthalmus (AR) | Neural tube defects |
| Chromosomal | Cleft lip/palate |
| 45, X | Sporadic |
| 6p– | Holoprosencephaly |
| 9q+ | Cornelia de Lange syndrome |
| Dup 5p | Goldenhar syndrome |
| Dup 8p | Kidney abnormalities |
| Dup 8q | Facial hemangiomas |
| Trisomy 9 | Klippel-Feil syndrome |
| Triploidy | Polysyndactyly |
| Dup 17q |
The landmark of the Dandy-Walker complex is the open fourth ventricle. This is demonstrated by sweeping the transducer in the posterior fossa along the axial plane and visualizing a fluid-filled tract connecting the cavity of the fourth ventricle to the cisterna magna (see Figure 8–1).5,6,13,19 In early gestation, this is a normal finding, as the developing cerebellar vermis has not yet completely enfolded the fourth ventricle.20,21 It is therefore imprudent to make a diagnosis of the Dandy-Walker complex at this gestational age, with the possible exception of those (rare) cases in which there is an obvious cystic enlargement of the cisterna magna or other abnormal findings.22 After 20 weeks, the vermis has normally “closed” the fourth ventricle; therefore, the demonstration of an opening is indicative of the Dandy-Walker complex.15,21
The varieties of the Dandy-Walker complex have much different prognostic implications An alarmingly high rate of erroneous diagnoses was reported in one series in which only axial transabdominal sonography had been used;1 this prompted a number of studies that have now established a systematic approach to the diagnosis involving multiplanar examinations possibly aided by magnetic resonance imaging (MRI).3,4,6,13,14 It is now well accepted that a specific diagnosis requires assessment of the vermis (absent, hypoplastic, or intact) and the torcular herophili (normal position or elevated).3,6,7 The evaluation of these findings is difficult and involves an element of subjectivity. There is potential for misinterpretation, particularly in early gestation, but an expert examiner using either sonography or MRI (or both) is able to make a precise diagnosis in the majority of cases.3,4
To assess the presence of the vermis, the best approach is to sweep the transducer in the posterior fossa along the axial plane. The vermis appears as an oval echogenic structure interposed between the fourth ventricle and the cisterna magna (see Figure 8–1). When this is not seen, and the area of the fourth ventricle is seen to communicate with the cisterna magna at any level, vermian agenesis can be inferred.
To assess the integrity of the vermis and the position of the torcular herophili, a median view is required. This can be obtained directly by multiplanar imaging, preferably through the posterior fontanelle, as this allows better visualization of the posterior fossa and brainstem. Three-dimensional ultrasound (3D US) can also be utilized.12,23 Indeed, one of the major shortcomings in the median view is the difficulty to obtain with absolute precision the exact plane of section and to confuse the cerebellar hemispheres with the vermis. The advantage of 3D US is the ability to control the sections using as reference the orthogonal planes. The use of volume contrast imaging may also facilitate visualization of subtle anatomical details.12,23 Once the vermis has been identified in the median plane, both a qualitative and a quantitative evaluation should be performed. It has been suggested that if the posterior apex (fastigium) of the fourth ventricle and the two main fissures of the vermis can be identified, the vermis is presumably intact.3,6,12,23,24,25 The secondary fissure is at times difficult to define in early gestation, and a semiquantitative approach can be used alternatively (normally, twice as much vermis is found below rather than above the primary fissure).6 Measurements of the fetal cerebellar vermis have been reported.26,27 Most cases of defective vermis involve agenesis of the caudal portion; therefore, the vertical diameter is probably the most relevant one. A small vermis with an abnormal configuration (absence of fastigium and/or fissure) indicates partial agenesis. Conversely, a small vermis with a normal configuration indicates hypoplasia.27 In practice, the distinction between these two entities in the fetus is difficult.
A word of caution is needed regarding the possibility of obtaining a truly, apparently normal median plane by two-dimensional (2D) or 3D US in a fetus with complete vermian agenesis as the cerebellar hemispheres may be displaced into the midline and be in contact with each other. In these patients, the coronal plane may be used to demonstrate that the vermis is absent and that the folia are abnormally oriented.27,28
Normally, the tentorium has a posterior inclination of roughly 45°, and the torcular herophili is implanted in the inner skull at the same level of neck muscles. In our experience, MRI is usually more effective than sonography in identifying the torcular herophili. The nuchal region is usually poorly visualized with US in the median plane because of acoustic shadowing, and one has to rely on the direction of the tentorium. A posterior inclination suggests a normal position, a horizontal direction, or a superior displacement. Upward dislocation of the tentorium indicates indirectly an enlargement of the cisterna magna that is usually found to exceed a depth of 10 mm.29,30 MRI has been advocated by many for the assessment of any cerebellar malformation identified with sonography.31
The Blake’s pouch cyst, which is by far the most frequent variety encountered prenatally, features an upward rotation of the cerebellar vermis (usually a slight one, < 45°). The cerebellar vermis, cisterna magna, and torcular herophili are in a normal position (Figures 8–5 and 8–6).3,6,12,14 Vermian hypoplasia/partial agenesis is identified by an upward displacement of a small vermis, whereas the cisterna magna and torcular herophili are normal (Figure 8–7).4,31 The landmark of the Dandy-Walker malformation is the large cisterna magna and the consequent superior displacement of the torcular herophili. The vermis is always significantly rotated superiorly (≥ 45°) and may be either normal or defective (Figures 8–8 and 8–9).4,6,7,16,24,25
Figure 8–5.
Sonography of Blake’s pouch cyst. (A) An axial scan demonstrates an open fourth ventricle (4v). (B) A coronal scan reveals that the vermis is present. (C) A sagittal scan demonstrates a seemingly intact and slightly rotated vermis. The cisterna magna is not enlarged. Downslanting of the tentorium suggests a normal insertion of the torcular herophili. (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

Figure 8–6.
MRI of Blake’s pouch cyst. When compared with the sonograms in the previous figures that were obtained from the same fetus, the most important contribution of MRI is the clear demonstration of the torcular herophili (TH) that is normally inserted. (Reproduced, with permission, from Atlas of Obstetric Ultrasound, 2009. The Global Library of Women’s Medicine. www.glowm.com.)

Figure 8–7.
Sonography of vermian hypoplasia. The fourth ventricle (4v) is open; the vermis is present but is about half the normal size and does not demonstrate any of the typical anatomical landmarks, the fastigium point and the main fissures. The cisterna magna is not enlarged. Downslanting of the tentorium suggests a normal insertion of the torcular herophili (TH). (Reproduced, with permission, from Atlas of Obstetric Ultrasound, 2009. The Global Library of Women’s Medicine. www.glowm.com.)

Figure 8–8.
Sonography of Dandy-Walker malformation showing an open fourth ventricle (4v), enlarged cisterna magna, superior rotation of the small dysmorphicvermis, and cranial displacement of the tentorium. (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

Figure 8–9.
MRI of fetal Dandy-Walker malformation. The information is similar to that provided with ultrasound in Figure 8–8. There is a better demonstration of the high-riding tentorium and torcular herophili (TH). (Reproduced, with permission, from the Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, International Society of Ultrasound in Obstetrics and Gynecology, 2010, www.isuog.org.)

It has been suggested that the shape of the opening of the fourth ventricle in the axial plane is relevant for the differential diagnosis of the different varieties of the Dandy-Walker complex.18 Also in our experience, an hourglass opening (“buttock” sign) is typical of the Blake’s pouch. A triangular or square-shaped opening is indicative of either vermian hypoplasia or Dandy-Walker malformation (see Figures 8–5, 8–7, and 8–8).
Other cerebral anomalies, including ventriculomegaly and agenesis of the corpus callosum, can be found, particularly with vermian hypoplasia/partial agenesis and Dandy-Walker malformation. Most frequently, a Blake’s pouch cyst is an isolated finding.12,13,32
The Dandy-Walker complex should be differentiated from other cystic anomalies of the posterior fossa. In cases of megacisterna magna, the cisterna magna is large, but the cerebellum is intact, and the fourth ventricle is triangular and closed.3,4,6,12 Cerebellar hypoplasia results in an ex vacuo large cisterna magna,33 but the main feature of the condition is a global reduction in the size of an otherwise normally shaped cerebellum4 (Figure 8–10). Arachnoid cysts growing in the posterior fossa have a mass effect and cause asymmetrical distortion of the cerebellum or pressure on the vermis, resulting in flattening of its dorsal border and in severe cases compression of the aqueduct and ventriculomegaly34 (Figure 8–11). The greatest difficulty encountered is posterior fossa hemorrhage, which results at times in destruction of the cerebellar vermis and enlargement of the cisterna magna, mimicking very closely a Dandy-Walker malformation or vermian hypoplasia (Figure 8–12).35
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


