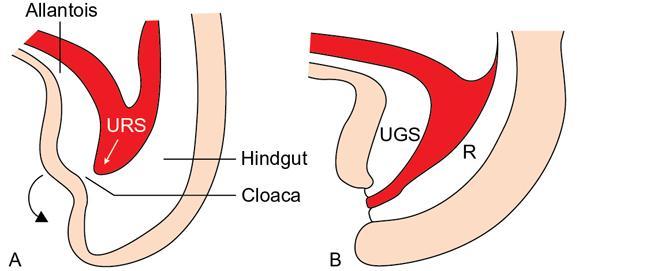
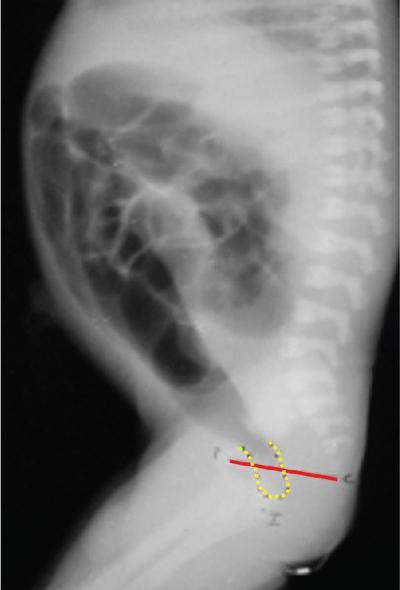
Arun Gupta, Manisha Jana, Devasenathipathy Kandasamy Anorectal malformations (ARM) are uncommon congenital malformations. They can either be found as an isolated anomaly or in association with other congenital malformations. The age of presentation and clinical presentation can have wide variation. In order to understand the complex anatomic details of the ARM, it is imperative to know the embryology and development of the normal anal canal. In the early embryonic life (4th–5th week), the primitive hindgut and the allantois communicate with each other at the cloaca. The membrane covering the cloaca at the caudal end is called cloacal membrane. During the 6th week of gestation, a sheet of mesenchyme (urorectal septum) grows between the allantois and hindgut. Eventually, lateral and midline folds develop in the cloaca, thereby dividing the common cavity into two parts: anteriorly urogenital sinus and posteriorly anorectum. Gradually, the embryo starts to lengthen and curve inwards. As a result, the distance between cloacal membrane and the tip of urorectal septum decreases and eventually, they meet each other. Consequently, the urogenital sinus and anorectum get completely separated (Fig. 7.6.1). In a later stage of gestation (7th–8th week), the anal canal gets secondarily occluded by epithelial plugs, which again gets recanalized to form the lower anal canal. Henceforth, it can be understood that any aberrations in the normal development at an earlier stage of gestation would result in a more severe degree and higher level of communication between urogenital system and anorectum. Any insult at a later stage of development will result in a low ARM, which will mostly have an abnormal anal opening in a normal position and no urogenital communication with the hindgut. Over the years, many classification systems for ARM have been introduced. Three major classifications are: Anorectal agenesis without fistula Anorectal agenesis with Rectal atresia Anorectal agenesis without fistula Anorectal agenesis with Rectal atresia H or N type fistula* Anal agenesis without fistula Anal agenesis with rectobulbar urethral fistula Anorectal stenosis Anal agenesis without fistula Anal agenesis with low rectovaginal fistula Anal agenesis with rectovestibular fistula Anorectal stenosis *Not described in original classification. #Site of anal opening is usually low but variable (1 and 2: at normal anal site; 3 and 4: at perineal site; 5–7: at vulvar location). Anorectal agenesis without fistula Anorectal agenesis with rectoprostatic urethral fistula Rectal atresia Anorectal agenesis without fistula Anorectal agenesis with rectovaginal urethral fistula Rectal atresia Anal agenesis without fistula Rectobulbar urethral fistula Anal agenesis without fistula Rectovaginal fistula Rectovestibular fistula Anal stenosis Anocutaneous fistula Anal stenosis Anocutaneous fistula Anovestibular fistula Rare Rare Anal or anorectal agenesis without fistula Rectal atresia Anal or anorectal agenesis Anal or anorectal agenesis without fistula Rectal atresia Cloacal anomalies Anal stenosis Imperforate anus without fistula Anal agenesis with rectoperineal fistula Anal stenosis Imperforate anus without fistula Anal agenesis with rectoperineal fistula Anal agenesis with rectovestibular fistula International classification was considered by some to be too detailed and too complex. However, in the authors’ experience, this system should ideally be followed in a high-volume teaching institute. A simplified version of it was, therefore, considered and is known by the name of Wingspread classification (so called because the meeting to decide it was held at the Wingspread convention centre in Racine, Wisconsin). More recently, another classification was proposed in the Krickenbeck conference on ARM in 2005. There are some common features/differentiating points in all the classification systems, namely the level of bling rectal pouch and presence/absence of fistula. Evaluation of a child with suspected ARM starts with a thorough clinical examination. Careful perineal examination should be performed to look for the number and location of the orifices. If an external anal orifice is appreciable, a low anomaly should be suspected. The location of anal orifice may be variable (Table 7.6.1). To the contrary, a flat perineum (no anal dimple or orifice) suggests a high anomaly. If there is evidence of meconium at urethral orifice/history of meconium in urine, it indicates presence of an internal fistula. In all suspected cases of high malformation, colostomy should be done, followed by detailed evaluation for the delineation of internal anatomy by contrast studies (discussed later). In the female child, if there is only one perineal opening, a cloacal malformation is likely. If two orifices are visible in the vulva with no anal orifice, then one of them is of the urethral, while the other one is of the vaginal orifice. Meconiun would come from the latter due to the associated recto-vaginal fistula. Colostomy is indicated in both the situations. If three orifices are visible, then two of them are respectively, of the urethra and the vagina, both at their normal site, while the third one is the bowel which could be at the normal anal site, or it might open as a fistulous track anteriorly at an abnormal site – either in the perineum or in the vestibule. Two most important investigations in the evaluation of ARM are invertography and contrast studies. Invertography is a procedure described back in 1930 by Wangensteen and Rice. This involved obtaining a lateral radiograph of the neonate, held upside down. An ideal time to obtain this radiograph is about 6–8 hours after birth, so as to allow the intestinal gas to reach the rectum. The thighs of the baby should be flexed, and X-ray beam should be centred at the greater trochanter. Anal dimple should be marked by barium paste. A properly done invertogram should have the following: On an invertogram, the distal part of the blind-ending bowel loop should be localized in relation to some specific bony landmarks, namely: Additional points to be evaluated on an invertogram are: presence/absence of spinal anomalies; and presence of gas in urinary bladder/vagina. Invertography is reported to be very accurate in differentiating a low-type fistula from intermediate/high type. However, the accuracy depends on how well the study has been performed. While interpreting invertogram, one must be aware of the pitfalls of this study (Table 7.6.4).
7.6: Anorectal malformations
Introduction
Embryology
Classification
Male
Female
High
Intermediate
Low #
Level
Male
Female
High
Intermediate
Low
Cloacal malformations
Type
Male
Female
Intermediate/High
Low
Evaluation of a child with arm
Clinical findings
Imaging evaluation
Invertography
Interpretation.
Study done too early (<6 hours after birth)
Bowel gas does not reach terminal part; falsely high level of anomaly on imaging
Meconium plugging the terminal bowel
False diagnosis of a high level of anomaly on imaging, as the gas does not reach terminal part
Excessive crying
Contraction of the puborectalis sling leads to a false diagnosis of a high level of anomaly on imaging
Presence of a patent fistula with urinary tract
Gas may escape through the fistula; delineating the level of anomaly might be difficult
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


