Answers to Unknown Case Sets
Case 1.1
- 1.1a.
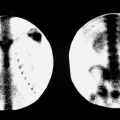
What is the most likely diagnosis? Unobstructed patulous collecting system of the right kidney with prompt washout of activity from the collecting system after Lasix.
- 1.1b.
If 370 MBq (10 mCi) of 99m TcO 4 − had been administered to the patient inadvertently instead of 99m Tc-MAG3, would this constitute a reportable “medical event”? No. An administration of a wrong radiopharmaceutical is reportable only if it causes an effective whole-body dose exceeding 0.05 Sv (5 rem) or 0.5 Sv (50 rem) to any organ. This does not occur with most diagnostic doses.
- 1.1c.
What is the difference in mechanism of renal excretion between DTPA and MAG3? DTPA is predominantly filtered whereas MAG3 is excreted by proximal tubules with minimal filtration (about 2%).
Case 1.2
- 1.2a.
What is the likely diagnosis?
- A.
Cortical atrophy with ventricular CSF reflux
- B.
Communicating arachnoid cyst
- C.
CSF leak
- D.
Ventricular shunt obstruction
- E.
Normal pressure hydrocephalus
- •
Answer E. Normal pressure hydrocephalus (NPH).
- A.
- 1.2b.
What characteristics differentiate this from a normal study? Prominent early ventricular entry with persistence and lack of “ascent” of activity over the cerebral convexities at 24 hours.
- 1.2c.
Identify the anatomy on these images. In this case, the heart-shaped central activity is abnormal entry into the bodies and anterior horns of the lateral ventricles. The bilateral adjacent foci are the inferior (temporal) horns of the ventricles. Activity immediately below this is in the basal cisterns. In normal patients, activity is seen on the anterior view as a trident with activity in the interhemispheric (central) and sylvian (bilateral) cisterns with no persistent ventricular activity.
Case 1.3
- 1.3.
Regarding the images, which of the following is/are true?
- A.
The results may be due to improper energy window setting.
- B.
Energy peaking is typically done using the activity in the patient.
- C.
The energy window should be 20% and centered at 160 keV.
- D.
A collimator defect was likely present on the posterior camera head.
- E.
The posterior camera head may be too far from the patient.
- •
Answers are A and E. The bone scan demonstrates loss of resolution on the posterior image. This may be caused by the posterior camera head being off-peak (not set for the correct energy window [140 keV] for 99m Tc), the posterior camera head being too far from the patient, or a camera electronic malfunction. Peaking is not typically done using activity in the patient due to excessive scatter.
- A.
Case 1.4
- 1.4a.
What is the finding? Gastrointestinal hemorrhage at the hepatic flexure of the colon. (Activity throughout the blood pool, including the heart, aorta, and iliac vessels, identifies this as a 99m Tc RBC scan.)
- 1.4b.
What bleeding rate is necessary to reliably detect the bleeding with angiography and scintigraphy? 1.0 mL/min with angiography and about 0.2 mL/min on scintigraphy.
- 1.4c.
If the study had been negative, what would be the next step in management? Imaging can be continued or, if the patient appears to be bleeding again within 24 hours after 99m Tc RBC administration, he or she can be returned for reimaging without reinjection, to assess for intermittent bleeding.
Case 1.5
- 1.5a.
What is the most likely diagnosis? Most cold thyroid nodules are due to colloid cysts, but about 10% to 20% may be thyroid cancer.
- 1.5b.
What is the differential diagnosis? A solitary cold nodule is a nonspecific finding. The common differential includes thyroid adenoma, colloid cyst, or thyroid cancer.
- 1.5c.
What is the next step in management? If not a simple cyst on ultrasound, fine-needle aspiration.
Case 1.6
- 1.6a.
What is the most likely diagnosis?
- A.
Dextrocardia
- B.
Breast attenuation artifact
- C.
Diaphragmatic attenuation artifact
- D.
Large anterior-apical infarct
- E.
Ischemic dilatation
- •
Answer D. Large anterior-apical infarct
- A.
- 1.6b.
Are there important ancillary findings? There is a severe fixed anterior-apical defect with the ventricular walls diverging toward the apex (the “trumpet sign”), consistent with aneurysm formation in a region of infarction.
- 1.6c.
What is the route of exctetion of 99m Tc-sestamibi? Biliary to bowel. Nearby liver, biliary, and bowel activity must be taken into account in timing the images to minimize artifacts. The organ receiving the highest dose is the gallbladder, or the colon if the gallbladder is absent.
Case 1.7
- 1.7a.
What is the most likely primary pathology? Lung cancer.
- 1.7b.
Is this patient amenable to surgery? No, because there are contralateral mediastinal metastases.
- 1.7c.
Is bronchioalveolar cancer (adenocarcinoma in situ) typically FDG-avid? No.
Case 1.8
- 1.8a.
What type of scan is this? A bone scan.
- 1.8b.
What is the most likely diagnosis?
- A.
Hepatic necrosis
- B.
Hepatitis
- C.
Budd-Chiari syndrome
- D.
Liver metastases
- •
Answer D. Multifocal or patchy diffuse uptake in an enlarged liver consistent with hepatic metastases. Hepatic necrosis could also be considered but is much less common. Mucinous tumors of the colon, ovary, and breast may calcify and have uptake.
- A.
- 1.8c.
What are some other causes of soft tissue uptake on bone scans? Infarcts, malignant ascites and malignant pleural effusions, lymphoma, lung cancer, meningioma, osteogenic sarcoma, dystrophic calcification, uterine fibroids, amyloidosis, dermatomyositis, calcific tendonitis, renal failure, hyperparathyroidism, mastitis, hematomas, and diffuse or focal soft tissue inflammation.
Case 1.9
- 1.9a.
Assuming the ventilation scan is normal and the chest radiograph shows hyperinflation, what is the probability of pulmonary embolism? Low probability for pulmonary embolism.
- 1.9b.
Does this appearance have a specific name? This is a “fissure sign” (right major and minor fissures) seen with pleural fluid or pleural thickening (often appearing in patients with COPD).
- 1.9c.
What is the “stripe” sign and what is its significance, if any? The stripe sign is different from the fissure sign. The stripe sign refers to a stripe of activity, between a perfusion defect and the pleura, indicating preserved perfusion in the subpleural lung. It is characteristic of COPD and without other significant findings indicates a very low probability of pulmonary embolism.
Case 1.10
- 1.10.
Regarding the image, which of the following is/are true?
- A.
The meter reading indicates that the package is likely damaged, and the delivery carrier and the NRC should be notified.
- B.
The radioactive II label means that this is a Type B package.
- C.
The limit for radiation dose at 1 meter from this package is 1 mrem (10 µSv) per hour.
- D.
A wipe test of the surface of this package is required upon receipt.
- E.
Such packages are required to be monitored within 3 hours of receipt or within the first 3 hours of the next business day.
- •
Answers C, D, and E are true.
- A.
Case 2.1
- 2.1a.
What is the most likely diagnosis?
- A.
Colon cancer metastasis
- B.
Tuberculosis
- C.
Lymphoma
- D.
Hemorrhagic stroke
- •
Answer C. 18 F-FDG-avid brain lymphoma seen as a homogeneously hypermetabolic mass.
- A.
- 2.1b.
How would an area of central necrosis have changed your diagnosis? An area of necrosis would be common in a high-grade astrocytoma.
- 2.1c.
How useful is this test in a patient with suspected CNS metastases from lung cancer? This would be a poor choice because most metastases are less metabolic than normal brain tissue and may not be apparent on FDG PET imaging. An enhanced MRI is the best test.
Case 2.2
- 2.2a.
What are the findings? Decreased activity in the frontal and frontotemporal regions on a 99m Tc-HMPAO SPECT brain scan.
- 2.2b.
What are the differential possibilities? These findings are characteristic of frontotemporal dementia (Pick disease) but can also be seen in schizophrenia, depression, and supranuclear palsy. Atypical Alzheimer disease may uncommonly present in this manner.
- 2.2c.
Does the distribution of activity represent regional metabolism or regional blood flow? HMPAO is a marker of regional blood flow, not metabolism.
Case 2.3
- 2.3a.
What is the most likely diagnosis?
- A.
Regenerating nodule
- B.
Focal nodular hyperplasia
- C.
Hepatoma
- D.
Hemangioma
- E.
Recent hematoma
- •
Answer C. Hepatoma. Gallium-67 is very sensitive for the detection of hepatocellular carcinoma. However, the test of choice if a hepatoma is suspected is a three-phase CT scan.
- A.
- 2.3b.
What other liver lesions may accumulate gallium? Abscess, lymphoma, and metastasis, with sensitivity varying with the primary tumor type .
- 2.3c.
What are appearances of hepatic adenoma and focal nodular hyperplasia on a 99m Tc-sulfur colloid liver scan? Adenomas will typically appear cold, whereas FNH typically has Kupffer cells and thus may appear to have the same activity as the liver or even increased.
Case 2.4
- 2.4a.
What type of scan is this? Hepatobiliary .
- 2.4b.
What is the diagnosis?
- A.
Bile leak
- B.
Free pertechnetate from poor radiopharmaceutical labeling
- C.
Biliary atresia
- D.
Choledochal cyst
- E.
Hepatitis
- •
The correct answer is E, neonatal hepatitis, as evidenced by the small bowel activity and inclusion of the entire body on the image indicating a neonate or small child. Premedication for 5 to 7 days with oral phenobarbital (2.5 mg/kg bid) may be used to improve hepatic excretion and test accuracy.
- A.
- 2.4c.
In an effort to keep radiation doses low to children, what administered activity should be given to this 2-kg infant? 1.0 mCi (37 MBq). Nobody expects you to memorize weight-specific doses in children, but you should know where to look them up. See Appendix D .
Case 2.5
- 2.5a.
What is the most likely diagnosis?
- A.
Shin splints
- B.
Hyperparathyroidism
- C.
Hypertrophic osteoarthropathy (HOA)
- D.
Renal failure
- E.
Bone contusion
- •
Answer C. Hypertrophic pulmonary.
- A.
- 2.5b.
Is there an incidental finding? Yes, right nephrectomy .
- 2.5c.
What other radiopharmaceutical can be used for bone scans besides 99m Tc-MDP? PET/CT bone scans can be done with 18 F-sodium fluoride. This radiopharmaceutical is very sensitive but has a several-fold higher cost and a sevenfold higher radiation dose than does MDP.
Case 2.6
- 2.6a.
What is the most likely diagnosis?
- A.
Fat emboli
- B.
Pneumonia
- C.
COPD
- D.
Metastases
- E.
Multiple thromboemboli
- •
Answer C. Chronic obstructive pulmonary disease (COPD). There are multiple matched ventilation/perfusion abnormalities bilaterally with delayed clearance of 133 Xe from the lungs.
- A.
- 2.6b.
What category is this according to PIOPED II criteria? Very low.
- 2.6c.
A large amount of central airway deposition on a 99m Tc-DTPA aerosol scan is an indication of what entity? COPD.
Case 2.7
- 2.7a.
What is the most likely diagnosis? Superscan with diffuse skeletal metastases.
- 2.7b.
Under what circumstances would you treat such a patient with 89 Sr-chloride or similar therapeutic radiopharmaceutical? Intractable bone pain with active blastic metastases should be present, and the WBC and platelet counts should be above 2400/µL and 60,000/µL, respectively. Optimally, renal function should be normal or the administered dose should be reduced to accommodate renal dysfunction, depending on its severity.
- 2.7c.
What radiation protection precautions are necessary after 89 Sr treatment? Because of beta (and no gamma) emission, few restrictions are necessary. Excretion is urinary and, to a lesser extent, fecal, which requires some instructions regarding frequency of urination to reduce bladder dose, sitting to urinate, and flushing the toilet twice afterward. Life expectancy should be at least 3 months because many states have restrictions on cremation, etc.
Case 2.8
- 2.8a.
What is the most likely diagnosis? Lymphoma based upon extensive adenopathy and multiple lung lesions. Other possibilities include metastatic melanoma and diffuse infection in an immunocompromised patient.
- 2.8b.
What is/are the main use(s) for FDG PET/CT in lymphoma? It is useful for staging, assessing treatment response and possible change of therapy, and detection of suspected recurrence.
- 2.8c.
Are MALT lymphomas typically FDG-avid? No .
Case 2.9
- 2.9a.
What is the most likely diagnosis? Multinodular goiter.
- 2.9b.
Is fine-needle aspiration biopsy warranted? In general, no, because the cold areas commonly are a result of nonfunctioning or poorly functioning adenomas and are much less likely to be cancer than is a solitary cold nodule. A dominant nodule, sonographically suspicious nodule, or MNG in a child deserves further characterization.
- 2.9c.
With what radiopharmaceutical was this scan performed? Significant activity in the salivary glands indicates that it was performed with 99m Tc-pertechnetate rather than 123 I.
- 2.9d.
In treating toxic MNG with 131 I, is the administered activity generally more or less than when treating Graves disease? More, largely because the lower, heterogeneously distributed uptake of radioiodine requires a larger dose.
Case 2.10
- 2.10a.
Is there a problem with delivery of this package containing radioactive material? Yes, it is not in a secured location, and the office almost certainly has no precautionary sign indicating “radioactive materials.”
- 2.10b.
What are the requirements concerning transport of a radioactive package? Material must be in an approved, usually Type A, container with a label indicating the transport index (TI) as well as the radiopharmaceutical and contained activity.
- 2.10c.
What are the requirements concerning acceptance? Packages must be secured, examined, monitored, and logged in. This procedure should be performed within 3 hours of receipt if it is received during normal working hours, otherwise within 3 hours on the next work day.
Case 3.1
- 3.1a.
What is the diagnosis? Bile leak with activity in the porta hepatis and right paracolic gutter.
- 3.1b.
Is the gallbladder present? No. In this case, the patient has had a recent cholecystectomy. Leaking bile commonly pools in the porta hepatis, gallbladder fossa, or around the liver (the “reappearing liver” sign). Obtaining a history of prior surgery is critical for accurate interpretation of the images.
- 3.1c.
What special views can be helpful? Right lateral decubitus and pelvic views can often be useful to search for bile flowing to other locations in the abdomen or pelvis.
Case 3.2
- 3.2a.
What is the most likely diagnosis? Brain death, as evidenced by no intracranial perfusion on the 99m Tc-pertechnetate study. The actual diagnosis of brain death should not be made by nuclear imaging tests alone but requires consideration of clinical parameters.
- 3.2b.
Can this study be done with 99m Tc-hexamethylpropyleneamine oxime (HMPAO)? Yes, although it is more costly than 99m Tc-pertechnetate or DTPA.
- 3.2c.
What would be the significance of sagittal sinus activity in a patient without obvious arterial phase activity? The significance is somewhat controversial, but most of the patients have a grave prognosis, and slight venous activity does not contradict the diagnosis of brain death.
Case 3.3
- 3.3a.
What is the most likely diagnosis?
- A.
Right renal artery stenosis
- B.
Right nephrostomy
- C.
Left obstruction
- D.
Left renal artery stenosis
- E.
Left patulous extrarenal pelvis
- •
The answer is C. Lasix renogram and time-activity curves demonstrating high-grade obstruction of the left kidney and a nonobstructed extrarenal pelvis on the right.
- A.
- 3.3b.
Could this study be done with 99m Tc-DMSA? No, DMSA is a renal cortical agent with essentially no urinary excretion.
- 3.3c.
After Lasix, how fast should the DTPA or MAG3 activity in a normal kidney decrease? Half should be excreted (the T1/2) in 7 to 10 minutes. A T1/2 longer than 20 minutes indicates obstruction. For suspected high-grade obstruction, MAG3 is preferred because of its tubular secretion component.
Case 3.4
- 3.4a.
What is the likely diagnosis? Stress fracture of third metatarsal.
- 3.4b.
Can osteomyelitis or an acute fracture have this appearance? Yes. Both can be “hot” on all three phases.
- 3.4c.
If this were an acute fracture, how long would increased activity be expected? For at least a few months and often up to a year.
Case 3.5
- 3.5.
Which of the following statements is/are true?
- A.
This image could represent a collimator damage artifact.
- B.
This appearance could be from a cracked crystal.
- C.
Flood fields should be done daily.
- D.
Flood fields can be done with either a sheet source or a point source.
- E.
“Salt and pepper” or “measles” appearance is indicative of moisture in the crystal.
- •
Answers B, C, D, and E are true.
- A.
Case 3.6
- 3.6a.
What is the most likely diagnosis? Graves disease.
- 3.6b.
Comparing 99m Tc-pertechnetate with 123 I for scanning, how is the radiopharmaceutical administered, and when should the patient be scanned? Intravenous administration and imaging at 15 to 30 minutes for 99m Tc-pertechnetate and oral administration and 3 to 24 hours imaging for 123 I.
- 3.6c.
If the 24-hour iodine uptake were 65% and the patient had known cardiac disease, would you treat this patient, and if so, how? The patient’s circulating thyroid hormone levels and TSH should be checked. The patient can be treated, usually with about 10 to 20 mCi (370 to 740 MBq); however, with such a medical history, it may be advisable to pretreat the patient with antithyroid medications.
Case 3.7
- 3.7a.
What is the most likely diagnosis? Small inferior and lateral left ventricular infarct with a large area of peri-infarct ischemia .
- 3.7b.
What vessels are involved? Circumflex and right coronary.
- 3.7c.
Where is the left ventricular apex on a bull’s eye (polar map) image? In the center .
Case 3.8
- 3.8a.
What is the most likely diagnosis?
- A.
Asthma
- B.
Pulmonary embolism
- C.
Lobar pneumonia
- D.
Mucous plug
- E.
Bullous emphysema
- •
Answer D. Left upper lobe focal air trapping with a smaller perfusion abnormality. In this case, it was due to a mucous plug. Other obstructing lesions such as lung cancer should also be considered.
- A.
- 3.8b.
In what projection is a 133 Xe scan typically performed, and why? In the posterior projection, because the energy of 133 Xe is relatively low and there is less attenuation of the photons by the heart and overlying soft tissue. Further, more pulmonary segments are assessed on the posterior image.
- 3.8c.
Where does the xenon go when the patient exhales? It should go into a xenon “trap,” which has a canister filled with activated charcoal. This needs to be replaced periodically. Exhaled xenon may also be exhaust-vented directly to the outside.
Case 3.9
- 3.9a.
What is the radiopharmaceutical used in this examination? 99m Tc-labeled red blood cells.
- 3.9b.
What is the most likely diagnosis?
- A.
Amoebic abscess
- B.
Cavernous hemangioma
- C.
Hepatoma
- D.
Focal nodular hyperplasia
- E.
Organizing hematoma
- •
Answer B. Hepatic cavernous hemangioma in the dome of the right lobe.
- A.
- 3.9c.
How would this entity appear on either a 99m Tc-sulfur colloid or 111 In-octreotide scan? Hemangiomas would be “cold” and have no activity on either scan.
Case 3.10
- 3.10a.
When are personnel dosimeters required in a nuclear medicine department? When there is a likelihood that an employee would be exposed to more than 10% of the occupational dose limit, dosimetry is required.
- 3.10b.
What are the annual occupational dose limits for the whole body and hands? 5 rem (50 mSv) effective dose for the whole body, and 50 rem (0.5 Sv) equivalent dose for the hands.
- 3.10c.
Do occupational dose limits include either background or personal medical exposure received by a technologist? No .
Case 4.1
- 4.1a.
What is the most likely diagnosis in this patient with a rising CEA? Colon cancer metastatic to the liver and para-aortic lymph nodes, as seen on an 18 F-FDG PET/CT scan.
- 4.1b.
What is the best test for suspected liver metastases from colon cancer? Contrast-enhanced MRI is the most sensitive, especially for small metastases.
- 4.1c.
What is the role of FDG PET/CT in staging colorectal cancer? Endoscopic ultrasound and endoscopy are best for assessing the primary tumor. PET/CT is valuable for assessing nodal and extranodal metastases, with PET being more sensitive than CT.
Case 4.2
- 4.2a.
What is the most likely diagnosis? Dilated cardiomyopathy with global hypokinesia.
- 4.2b.
What is the top normal left ventricle (LV) end-diastolic volume on gated-SPECT myocardial perfusion images? The value used is somewhat variable and dependent on technique/software used, but generally more than 120 to 130 mL is considered abnormal.
- 4.2c.
What does myocardial uptake of the PET imaging agents 13 NH 3 and 82 Rb map? The presence and distribution of myocardial perfusion.
Case 4.3
- 4.3a.
What is the most likely diagnosis in this patient who was in an auto accident 5 years earlier? Splenosis.
- 4.3b.
What radiopharmaceutical besides 99m Tc-sulfur colloid can be used to make this diagnosis? 99m Tc heat-damaged red blood cells, which are also phagocytized by the Kupffer cells.
- 4.3c.
What other entities can cause nonvisualization of the spleen on a 99m Tc-sulfur colloid scan? Congenital asplenia and post-splenectomy status, sickle cell disease (autosplenectomy), and functional asplenia.
Case 4.4
- 4.4a.
What is the most likely diagnosis? High probability for pulmonary embolism.
- 4.4b.
What is the approximate number and size of 99m Tc-MAA particles administered? About 400,000 particles, with most particle diameters between 10 and 30 µm.
- 4.4c.
If this patient has pulmonary hypertension, what is the likelihood that pulmonary emboli are the cause, and why is this information important? With pulmonary hypertension and a high-probability scan, there is a 95% chance that the hypertension is due to PE and may be surgically treatable with thromboendarterectomy, which is not the case for other etiologies.
Case 4.5
- 4.5a.
What is the most likely diagnosis?
- A.
Prostate metastases
- B.
Trauma
- C.
Paget disease
- D.
Chronic osteomyelitis
- E.
Multiple osteochondromas
- •
Answer C. Polyostotic Paget disease.
- A.
- 4.5b.
What are the pertinent associated findings on the pelvis radiograph? Expansion of the left iliac wing and ischial sclerosis.
- 4.5c.
Do the lytic lesions associated with Paget disease show increased radionuclide uptake on a bone scan? Yes.
Case 4.6
- 4.6a.
What is the most likely diagnosis? Acute tubular necrosis (ATN).
- 4.6b.
Could dehydration produce the same pattern? Yes.
- 4.6c.
Would chronic renal disease produce the same pattern? No. With chronic renal disease, there is slow clearance of activity from the soft tissues and slow uptake and excretion in the renal parenchyma.
Case 4.7
- 4.7a.
What type of scan is this? Iodine-131 MIBG. There are clearly focal skeletal abnormalities. The poor statistical quality and resolution suggest a high-energy radionuclide consistent with an 131 I-labeled agent. A sodium 131 I scan would not have liver and spleen activity.
- 4.7b.
What is the most likely diagnosis?
- A.
Kaposi sarcoma
- B.
Prostate cancer with metastases
- C.
Multifocal osteomyelitis
- D.
Pheochromocytoma with metastases
- E.
Adrenal adenocarcinoma with metastases
- •
Answer D. Pheochromocytoma with osseous metastases.
- A.
- 4.7c.
What other pathologic entities show increased activity with this radiopharmaceutical? Carcinoid, neuroblastoma, medullary thyroid carcinoma, and paraganglioma.
Case 4.8
- 4.8a.
What is the likely diagnosis? Lymphoma.
- 4.8b.
What is the significance of the splenic activity? The stage is at least III S.
- 4.8c.
What is the size threshold for detection of a lesion on FDG PET? About 6 mm.
Case 4.9
- 4.9a.
What is the most likely diagnosis?
- A.
Medullary thyroid cancer
- B.
Hürthle cell thyroid cancer
- C.
Parathyroid adenoma
- D.
Autonomous nodule
- E.
Discordant nodule
- •
Answer E. Discordant nodule “hot” on 99m Tc-pertechnetate scan and “cold” on radioiodine scan.
- A.
- 4.9b.
Does this finding warrant further follow-up? Yes. A small number of these are thyroid carcinomas.
- 4.9c.
On the 99m Tc-pertechnetate RAO image, what is the activity below the thyroid gland? 99m TcO 4 − in swallowed saliva. How can you be sure? This can be checked by having the patient drink water and then reimaging.
Case 4.10
Which of the following statements is/are true regarding pregnancy and radiation exposure?
- A.
A pregnant nuclear medicine technologist should wear two lead aprons.
- B.
The dose limit for the embryo/fetus only applies after the pregnancy is declared.
- C.
The fetal thyroid does not accumulate radioiodine until about 10–12 weeks gestation.
- D.
Radioiodine easily passes across the placenta and into breast milk.
- E.
A pregnant technologist cannot be allowed to perform a PET/CT scan.
- •
Answers B, C, and D are true. A pregnant technologist or physician can be actively involved with nuclear medicine patients as long as dose limits are not exceeded.
- A.
Case 5.1
- 5.1a.
What is the most likely diagnosis?
- A.
Alzheimer dementia
- B.
Lewy body dementia
- C.
Multi-infarct dementia
- D.
Huntington disease
- E.
Pick disease
- •
Answer A. Alzheimer disease, as evidenced by symmetrically decreased metabolism in the parietotemporal regions bilaterally.
- A.
- 5.1b.
What are the expected findings in Lewy body dementia on 18 F-FDG PET imaging? Changes similar to Alzheimer disease but with occipital involvement more likely. Loss of dopaminergic activity in the striatum on 123 I-ioflupane imaging also favors Lewy body dementia.
- 5.1c.
What is crossed cerebellar diaschisis and is it present in this patient? It is typically seen as hypometabolism in the cerebellar hemisphere contralateral to a supratentorial cerebral lesion such as tumor, stroke, or trauma. It is not present in this patient .
Case 5.2
- 5.2a.
What is the major finding? Hydronephrosis and markedly dilated bladder.
- 5.2b.
What is the likely cause? Transitional cell carcinoma, as evidenced by the irregular mass near the uterovesicular junction.
- 5.2c.
What is the value of 18 F-FDG PET in this entity? FDG PET is of limited value because a large percentage of renal and bladder cancers do not appreciably accumulate FDG, and urinary excretion of 18 F-FDG hinders visualization. FDG PET/CT is more valuable for the detection of regional and distant metastases than in the evaluation of the primary tumor.
Case 5.3
- 5.3a.
What is the most likely diagnosis? The study is abnormal on all three phases of the bone scan as evidenced by markedly increased activity along the entire shaft length. While an infected long-stem right hip prosthesis is likely, the findings are not specific.
- 5.3b.
What other nuclear medicine techniques are more appropriate in this setting? 111 In-leukocyte scan combined with 99m Tc-sulfur colloid marrow imaging is the procedure of choice for suspected prosthetic joint infections, especially in the case of an equivocal bone scan.
- 5.3c.
What pattern is often seen on MDP scans with hip prosthesis loosening? While increased activity at the tip of the shaft and near the lesser trochanter are the sites with the most stress and motion as a result of loosening, the findings are not specific, and further imaging is warranted as previously noted.
Case 5.4
- 5.4a.
What type of examination is this? 99m Tc-sestamibi parathyroid scan.
- 5.4b.
What is the most likely diagnosis? Ectopic mediastinal parathyroid adenoma.
- 5.4c.
What other entities might this represent? Other primary tumors such as thyroid and parathyroid cancers, thymomas, and even benign fibroadenomas may present in this manner, as well as various metastatic lesions.
Case 5.5
- 5.5a.
What is the most likely diagnosis?
- A.
Temporal lobe epilepsy
- B.
Low-grade glioma
- C.
High-grade glioma
- D.
Stroke with luxury perfusion
- •
Answer B. 18 F-FDG PET/MRI scan demonstrating low metabolic activity consistent with a low-grade temporal glioma.
- A.
- 5.5b.
What findings would be expected on 201 Tl and 99m Tc-HMPAO brain scans done to distinguish recurrent tumor from radiation necrosis? Both entities would show decreased HMPAO activity, but with recurrent tumor, thallium activity is focally increased.
- 5.5c.
What is the significance of interval increasing 18 F-FDG activity in an area of a previously known low-grade glioma? This would suggest anaplastic transformation. FDG activity in primary brain tumors generally correlates inversely with survival.
Case 5.6
- 5.6a.
What is the most likely diagnosis? This patient had a cavitary squamous cell lung cancer with rib involvement, as seen on an 18 F-FDG PET/CT scan. A large lung abscess could also appear in this manner.
- 5.6b.
What is the hot spot in the right supraclavicular region? This was an attenuation correction artifact caused by the cardiac pacing device seen on the chest radiograph.
- 5.6c.
Which set of images is not attenuation corrected? The lower row of images is not attenuation corrected as evidenced by the prominent diffuse skin activity and the absence of the attenuation correction pacemaker artifact.
Case 5.7
- 5.7a.
What is included in the differential diagnosis? In this case, markedly reduced trapping of the radiopharmaceutical is a result of subacute thyroiditis (De Quervain thyroiditis) as seen on this 99m Tc-pertechnetate scan (note the prominent salivary, blood pool, and background activity). This may also be seen in patients receiving thyroid hormone replacement, ectopic endogenous thyroid hormone production (such as “struma ovarii”), or primary or secondary hypothyroidism.
- 5.7b.
Would this pattern likely be due to prior stable iodine ingestion? No. While that would reduce uptake on a radioiodine scan, it has little effect on trapping of 99m Tc-pertechnetate scan.
- 5.7c.
What scan patterns might be seen with chronic forms of thyroiditis? The scintigraphic presentation of chronic thyroiditis is very variable and can have diffusely uniform increased activity (mimicking Graves disease), coarsely patchy distribution (mimicking a multinodular gland), generally decreased activity, or even a normal appearance. Thyromegaly is usually the presenting clinical finding.
Case 5.8
- 5.8a.
What is the most likely diagnosis? LV anteroseptal myocardial ischemia.
- 5.8b.
What would be the implications if the left ventricle cavity appeared dilated on the stress images? In the presence of CAD, transient ischemic dilatation (TID) correlates with high-risk disease (left main or multivessel involvement) and a worse prognosis.
- 5.8c.
What is the mechanism of transient ischemic dilatation? Underlying mechanisms for transient ischemic dilatation include transient stress-induced diffuse subendocardial hypoperfusion, producing an apparent cavity dilatation, ischemic systolic dysfunction, and perhaps in some instances, physical cavity dilatation.
Case 5.9
- 5.9a.
Assuming a normal chest radiograph, what is the diagnosis? The normal ventilation with diffuse bilateral, multiple small perfusion defects is nonspecific. In this case, the diagnosis is diffuse vasculitis.
- 5.9b.
What modified PIOPED II probability category would this represent? Low.
- 5.9c.
What is the differential diagnosis in this case? Fat or tumor emboli could have a similar appearance.
Case 5.10
- 5.10a.
What methods are commonly used for disposal of radioactive syringes? Either return to the commercial radiopharmacy that supplied the material or decay in storage.
- 5.10b.
Is the method shown here appropriate? No, there is no radioactive label visible on the container.
- 5.10c.
How long is storage required? Can only be done for byproduct material with half-lives of less than 120 days. These materials should be stored for 10 half-lives at which time the measured dose rate is indistinguishable from background. Radioactive labels are then removed before disposal with ordinary waste. Decay and disposal records must be maintained.
Case 6.1
- 6.1a.
Is this likely to represent chronic cholecystitis? No, the linear activity that accumulates in the pericholecystic liver parenchyma of the right lobe is the “rim sign,” indicative of acute cholecystitis.
- 6.1b.
Is there a need to alert the clinician, and if so, why? Yes. About 40% of patients with the rim sign have an abscessed or gangrenous gallbladder.
- 6.1c.
Is there an advantage to slow infusion of CCK over more than 10 minutes in performing a gallbladder ejection fraction study? Yes, the patient is likely to have less abdominal discomfort than with rapid injection. Be aware that normal gallbladder ejection fraction values vary, depending on the infusion duration.
Case 6.2
- 6.2a.
What is the most likely diagnosis? Infected axillary-femoral graft. Incidental note of right nephrectomy.
- 6.2b.
What criteria should be used in making the diagnosis? 18 F-FDG scanning should not be used in cases of suspected graft infection within the first 2 to 4 months of surgical placement as inflammation due to residual healing may produce a false-positive study. Inhomogeneous, mild, or moderate uptake should be considered as nondiagnostic. FDG has good sensitivity (about 90%) but poor specificity (about 60%) for the diagnosis of graft infection.
- 6.2c.
What is the value of 99m Tc-WBC compared with FDG PET/CT in this setting? 99m Tc-WBC is more specific for infection than is FDG PET/CT.
Case 6.3
- 6.3a.
What is the most likely diagnosis?
- A.
Aneurysmal bone cysts
- B.
Multiple enchondromas
- C.
Healing rib fractures
- D.
Fibrous dysplasia
- E.
Multiple bone infarcts
- •
Answer D. Fibrous dysplasia, as seen on a radionuclide bone scan, and expansile lesions on rib radiograph.
- A.
- 6.3b.
Are multiple enchondromas typically “hot” on a bone scan? Yes .
- 6.3c.
What are physiologic factors that cause increased activity on bone scans? Increased osteoid formation, increased blood flow, increased mineralization of osteoid, and interrupted sympathetic nerve supply.
Case 6.4
- 6.4a.
What is the most likely diagnosis? Parathyroid adenoma, as seen on a 99m Tc-sestamibi scan .
- 6.4b.
Could this lesion be an atypical thyroid adenoma? Very unlikely, because on the SPECT/CT, it is separate from the thyroid gland.
- 6.4c.
What method could be used to help locate the lesion at surgery? Often a small gamma probe is used during surgery, but the patient needs to receive 99m Tc-sestamibi 2 to 4 hours before surgery.
Case 6.5
- 6.5a.
What is the most likely diagnosis?
- A.
Aspergillosis
- B.
Small cell lung cancer
- C.
Lymphoma
- D.
Bronchoalveolar carcinoma (adenocarcinoma in situ)
- •
Answer A. Aspergillosis, although lung cancer should be considered in the differential diagnosis on this 18 F-FDG PET/CT scan.
- A.
- 6.5b.
Is metastatic disease present? There are multiple hypermetabolic ipsilateral hilar and mediastinal lymph nodes. In this case, these were a result of infected or reactive lymph nodes, not metastasis.
- 6.5c.
What is the role of 18 FDG PET/CT in infection? FDG is very sensitive for the detection of both infection (especially granulomatous) and inflammation; however, it is very nonspecific. Hyperplastic and neoplastic lymph nodes may also be hypermetabolic. 18 F-FDG is useful for the evaluation of FUO, sarcoidosis, and vascular graft infection. It is generally better than 67 Ga-citrate in these settings.
Case 6.6
- 6.6a.
What is the most likely diagnosis? Reversible ischemia of the septum, anterior wall, apex, and distal inferior wall with septal dyskinesia, as seen on a gated 99m Tc-sestamibi scan using exercise stress.
- 6.6b.
What parameters are used to determine if physical exercise stress was adequate in this patient? The determination of peak stress varies with the institution, but it is generally considered to be maximal when chest pain or significant ECG changes appear, when the patient’s heart rate reaches 85% of the predicted maximum heart rate (frequently defined as 220 beats/min minus the patient’s age in years), or when the heart rate–blood pressure product (maximum heart rate achieved multiplied by the maximum systolic blood pressure) exceeds a value of 25,000. If none of these conditions is met, the stress is generally deemed submaximal.
- 6.6c.
What degree of coronary artery stenosis is important? When the narrowing of a coronary artery diameter is less than 50% of the diameter of the vessel, the effect on blood flow generally is clinically insignificant. As diameter narrowing approaches 70%, the lesions become much more hemodynamically significant, particularly during exercise. To be significant at rest, 90% or greater narrowing is usually required.
Case 6.7
- 6.7a.
What is the most likely diagnosis? Lytic sternal metastasis, as seen on a 99m Tc bone scan.
- 6.7b.
What cancer types often produce predominantly lytic bone metastases? Kidney, lung, thyroid .
- 6.7c.
What tumor type most often causes single sternal metastases? Breast cancer.
Case 6.8
- 6.8a.
What is the most likely diagnosis? Toxic thyroid adenoma, as visualized on a 99m Tc-pertechnetate thyroid scan.
- 6.8b.
Could this lesion be malignant? Yes. Although exceedingly rare (less than 1%), nodules that are hot on 99m Tc-pertechnetate scans can be thyroid cancer. A thyroid cancer would not be hotter than the normal thyroid tissue on a 123 I scan.
- 6.8c.
Does the remainder of the gland appear normal? No. The activity in the rest of the gland is decreased because of the autonomous nodule producing too much hormone and inhibiting pituitary production of circulating TSH.
Case 6.9
- 6.9a.
What is the most likely diagnosis? Pneumonia.
- 6.9b.
What is meant by the term “triple match”? The term triple match is often used to refer to matched ventilation/perfusion abnormalities accompanied by a corresponding chest radiographic abnormality of the same size, usually, but not always, an airspace opacity.
- 6.9c.
What probability of PE is associated with a triple match? Matching ventilation/perfusion defects corresponding to chest radiographic opacities isolated to the upper and middle lung zones imply a very low (less than 10%) probability of pulmonary embolus, whereas similar findings in the lower lung zones represent an intermediate or moderate (20% to 80%) probability of pulmonary embolus.
Case 6.10
- 6.10.
Regarding the administration of the material shown in the image, which of the following is/are true?
- A.
According to the NRC, the patient must be hospitalized after administration.
- B.
A written directive is required for any administration of 131 I.
- C.
The procedure must be supervised by the radiation safety officer (RSO).
- D.
Criteria for patient release can be measured with a survey meter.
- E.
It is recommended that the patient not travel home using public transportation.
- •
Answer E is true. Answers A, B, C, and D are not true for the following reasons:
- •
A. Not all patients treated with high doses of 131 I need to be hospitalized. Release of nuclear medicine patients is allowed under NRC regulations, based on a certain amount of administered activity or dose rate (e.g., 33 mCi [1.2 GBq] or less of 131 I or 7 mrem [70 µSv]/hr or less at 1 meter for 131 I). Patients also may be released with much higher activities, based on patient-specific calculations and if the effective dose to family or caregiver is not likely to exceed 0.5 rem (5 mSv).
- •
B. A written directive for 131 I sodium iodide administration is only needed for dosages exceeding 30 µCi (1.1 MBq).
- •
C. An authorized user must complete and sign the written directive for therapy, but no RSO supervision is required.
- •
D. An ionization chamber instrument is used to assess whether a patient meets the criteria for release.
- •
- A.
Case 7.1
- 7.1a.
What is the most likely diagnosis? Right-to-left shunt on a 99m Tc-MAA lung perfusion scan.
- 7.1b.
If you suspected such a shunt was present, should you have done this procedure at all or modified the procedure? It is common practice to limit the number of particles in the presence of a right-to-left shunt from about 400,000 to about 100,000.
- 7.1c.
What causes “hot spots” in the lung on a 99m Tc-MAA perfusion scan, and are they clinically significant? Withdrawal of blood into the syringe containing 99m Tc-MAA before injection may result in labeling of small clots or clumping of the MAA. Once injected, they lodge in the pulmonary capillary bed, causing “hot spots” that are not clinically significant.
Case 7.2
- 7.2a.
What type of scan is this? Hepatobiliary scan, as evidenced by the sequential images, initial cardiac blood pool activity that gets cleared by the liver, and no visualization of the spleen.
- 7.2b.
What is the diagnosis? “Liver scan” sign as a result of intrahepatic cholestasis (hepatitis) or acute/subacute common bile duct obstruction (usually a stone).
- 7.2c.
Is this radiopharmaceutical conjugated by the liver? No, in contrast to bile, iminodiacetic acid agents are not conjugated before excretion.
Case 7.3
- 7.3a.
What is the most likely diagnosis? Hyperparathyroidism with 99m Tc-MDP activity in the lungs, thyroid, kidneys, and stomach as a result of so-called metastatic calcification.
- 7.3b.
What are the two common bone scan presentations of this entity? (1) Increased activity in the skull, extremities, and around the large joints; and (2) soft-tissue activity in the lungs, kidneys, thyroid, stomach, and/or pancreas.
- 7.3c.
What are common clinical symptoms and findings associated with this entity? Nephrolithiasis, weakness, fatigue, and bone and joint pain (sometimes referred to as “stones, bones, and groans”).
Case 7.4
- 7.4a.
What is the most likely diagnosis? Inferior wall myocardial wall infarction with severe inferior wall hypokinesis.
- 7.4b.
What is hibernating myocardium? Hibernating myocardium is the result of chronic hypoperfusion and ischemia. This leads to reduced cellular metabolism that is sufficient to sustain viability but inadequate to permit contractile function. Areas of hibernating myocardium usually present as segments of decreased perfusion and absent or diminished contractility.
- 7.4c.
What is stunned myocardium? Stunning is the result of ischemic and reperfusion injury secondary to an acute coronary artery occlusion that has reopened before significant myocardial infarction can occur. Areas of stunned myocardium usually present with normal or near-normal perfusion but with absent or diminished contractility, which often improves spontaneously over time.
Case 7.5
- 7.5a.
What is the most likely diagnosis? Bilateral renal artery stenosis.
- 7.5b.
What is the mechanism by which captopril works? In renal artery stenosis, the efferent blood vessels constrict to maintain filtration pressure in the glomeruli. After administration of an ACE inhibitor, the efferent renal blood vessels become dilated, reducing glomerular filtration pressure with the affected kidney(s) retaining activity in the tubules because of diminished washout of the tubular activity. Thus, when 99m Tc-MAG3 is used, the affected kidney(s) presents as a persistent “nephrogram” after captopril is administered.
- 7.5c.
Is known severe renal artery stenosis a relative contraindication to this procedure? Yes, the drop in intrarenal blood pressure from captopril can induce acute renal failure.
Case 7.6
- 7.6a.
What are the findings? Decreased metabolic activity in the left temporal lobe at the site of the seizure focus.
- 7.6b.
What is the differential? This is a case of interictal (between seizures) temporal lobe epilepsy, but similar findings can be seen with a low-grade temporal tumor, stroke, or radiation necrosis.
- 7.6c.
What pattern of metabolism or perfusion is seen with imaging during a seizure (ictal imaging)? Increased activity at the site of seizure focus .
Case 7.7
- 7.7a.
What is the most likely diagnosis? Lingual thyroid, as seen on a 99m Tc-pertechnetate thyroid scan .
- 7.7b.
What is the usual thyroid function status in these patients? About 70% of these patients are hypothyroid, and 10% have significant accompanying mental and physical impairments of congenital hypothyroidism (cretinism).
- 7.7c.
What is the pathogenesis of this entity? Embryologically, thyroid tissue originates near the base of the tongue and migrates caudally. But when the migration is arrested, ectopic positioning results, commonly at the base of the tongue, producing a lingual thyroid gland.
Case 7.8
- 7.8a.
Is this a GI bleeding study? No. It is a Meckel diverticulum study using 99m Tc-pertechnetate, as evidenced by the prompt gastric wall activity and minimal blood pool activity.
- 7.8b.
Does a negative result mean that there is no Meckel diverticulum present? No. A Meckel diverticulum can still be present. However, it does mean that ectopic gastric mucosa is not likely to be present, which is generally the cause of bleeding.
- 7.8c.
What premedication(s) can increase the sensitivity of this procedure? H 2 blockers (cimetidine) reduce the release and washout of pertechnetate from ectopic gastric mucosa, pentagastrin can enhance gastric mucosal uptake, and glucagon decreases contractility movement during imaging.
Case 7.9
- 7.9a.
What is the most likely diagnosis? Multivessel coronary artery disease. Large anteroapical infarct with akinesis, small inferior wall infarct, reduced left ventricle (LV) ejection fraction, and dilated LV.
- 7.9b.
What are the adverse reactions associated with dipyridamole pharmacologic stress, and how are they treated? Dipyridamole may cause chest discomfort, headaches, dizziness, flushing, and nausea. These side effects may be rapidly reduced by the intravenous administration of aminophylline (100 to 200 mg). This antidote should be readily available during the procedure. Aminophylline is also used to reverse the effects of the widely used vasodilator regadenoson.
- 7.9c.
What are the side effects and method of treatment for adverse reactions to adenosine stress? Side effects with adenosine are more common than those with dipyridamole and occur in 75% of patients. The three most common side effects are flushing, shortness of breath, and chest pain. These are usually transient and require no action or treatment. An uncommon, but more serious, side effect is atrioventricular block, which usually occurs in the first few minutes of infusion and is also transient. First-degree and second-degree block are more common. Because the biologic half-life of adenosine is extremely short (less than 10 seconds), its effects may be reversed by simply stopping infusion and beginning any specific treatments, if necessary.
Case 7.10
- 7.10.
If the flask contained 111 MBq (3 mCi) of 131 I, which of the following is/are correct?
- A.
This is classified as a major spill.
- B.
This spill could be managed without involving the RSO.
- C.
Potassium iodide should be considered if the liquid got on the skin.
- D.
Contaminated skin should be treated with scrubbing until survey counts indicate normal background levels.
- E.
A report to the NRC may be required.
- •
Answers A, C, and E are correct.
- •
This is classified as a major spill (greater than 1 mCi [37 MBq] of 131 I). See Appendix I and Table I.1 .
- •
For a major spill, the RSO must be notified and involved. Nonaffected persons should vacate the area, the spill should be covered to prevent spread (do not attempt to clean up), and the area secured. Contaminated persons should remove affected clothing and wash with soap and warm water. Scrubbing to background activity is not necessary.
- •
With radioiodine, the authorized user and RSO may consider giving potassium iodide as a thyroid blocking agent and later doing either urine or thyroid counts to assess possible internal contamination for affected persons.
- •
- A.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


